Abducens Neurovascular Conflict¶
Summary
- Vascular compression of CN VI causing horizontal diplopia from lateral rectus palsy
- The offending vessel contacts the nerve at its root exit zone or cisternal (prepontine) segment
- High-resolution 3D T2 (CISS/FIESTA/DRIVE) demonstrates the neurovascular contact and any nerve distortion1
Pathophysiology¶
- Pulsatile arterial compression causes focal demyelination and axonal injury of CN VI
- Common offending vessels: AICA, basilar artery, vertebral artery (often dolichoectatic) and SCA
- Contact is usually at the root exit zone (pontomedullary junction) or within the prepontine cistern
Demographics¶
- Rare; most often adults 40–70 years, with no clear sex predilection
- Associations: hypertension, atherosclerosis and vertebrobasilar dolichoectasia
Diagnosis¶
- Horizontal diplopia worse on lateral gaze, esotropia and failure of abduction, without other cranial neuropathies
- Requires a clinical CN VI palsy plus MRI neurovascular contact, having excluded other causes
Imaging¶
- High-resolution 3D heavily T2-weighted sequences (CISS/FIESTA/DRIVE), ≤1 mm, are the mainstay
- Show the vessel contacting, displacing or indenting the cisternal nerve
- TOF-MRA identifies the offending vessel and any dolichoectasia for surgical planning
- Chronic compression may cause nerve atrophy; secondary lateral rectus denervation/atrophy may be seen
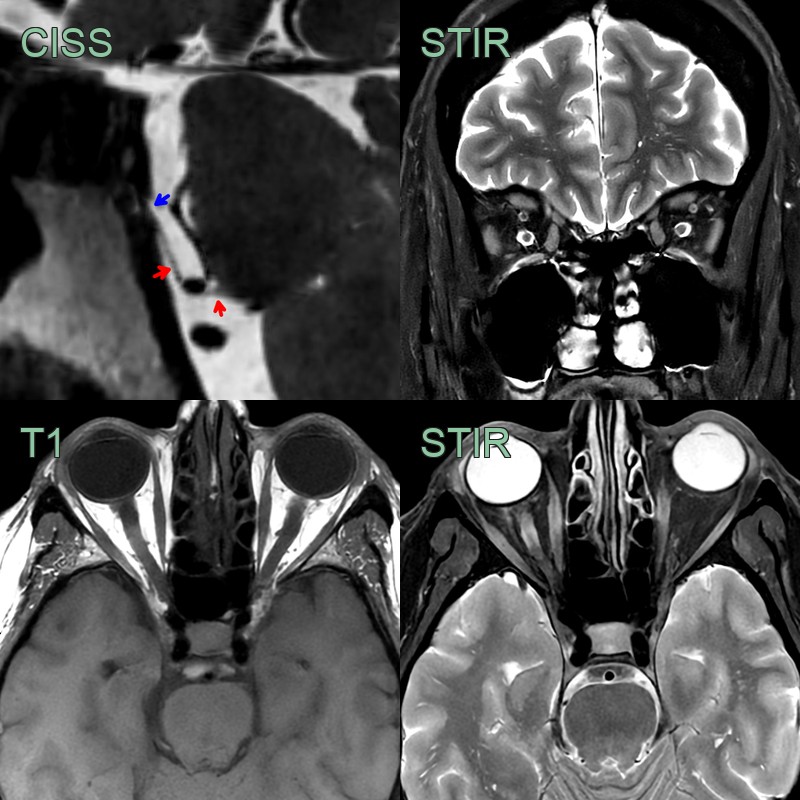
- A 40-year-old patient presented with a progressive left abducens palsy.
- MRI showed the cisternal segment of the abducens nerve (red) distorted by the AICA before entering Dorello's canal.
- The left lateral rectus muscle was subtly T2-hyperintense and atrophic.
Treatment¶
- Conservative first-line: observation (spontaneous resolution possible), prisms, botulinum toxin
- Microvascular decompression is reserved for persistent, disabling symptoms
Differential diagnosis¶
| Imaging differential | Differentiating feature |
|---|---|
| Abducens schwannoma | Enhancing fusiform mass along the cisternal nerve or Dorello's canal, rather than a vascular loop |
| Petroclival / Dorello's canal meningioma | Enhancing dural-based mass with a dural tail |
| Vertebrobasilar dolichoectasia | Ectatic tortuous vessel contacting the nerve; asymptomatic contact is common, limiting specificity |
| Petrous apex lesion (cholesterol granuloma, apical petrositis) | Expansile petrous apex lesion abutting Dorello's canal |
| Cavernous sinus lesion | Mass or abnormal enhancement in the cavernous sinus affecting the intracavernous CN VI |
-
Elder et al. Isolated Abducens Nerve Palsy: Update on Evaluation and Diagnosis. 2016. Current neurology and neuroscience reports - Open in new tab. ↩