Acute Disseminated Encephalomyelitis (ADEM)¶
Summary
- Acute inflammatory demyelinating disorder of the central nervous system
- Typically follows viral infection or vaccination
- Characterised by multifocal white matter lesions1
Pathophysiology¶
- Autoimmune-mediated demyelination
- T-cell mediated response against myelin basic protein
- Perivascular inflammation and oedema in white matter
- Grey matter involvement can occur, particularly in the thalamus and basal ganglia
Demographics¶
- More common in children and young adults
- Peak incidence between 3-10 years of age
- Slight male predominance (1.3:1)
- Incidence: 0.3-0.6 per 100,000 person-years
Diagnosis¶
- Clinical presentation:
- Acute onset of neurological symptoms (encephalopathy, motor deficits, ataxia)
- Often preceded by viral illness or vaccination (1-4 weeks prior)
- Cerebrospinal fluid analysis:
- Mild pleocytosis
- Elevated protein
- Oligoclonal bands (less common than in multiple sclerosis)
- Neuroimaging
- Characteristic lesions as described below
- Exclusion of other neurological disorders
Imaging¶
- CT:
- Hypodensities in the same distribution as the T2-weighted hyperintensities described below.
-
MRI
- T2: Multiple, large (>1-2 cm) hyperintense lesion white matter (deep grey nuclei may be involved)
- T1+C: Variable. May be absent initially. When present, usually peripheral or leading edge enhancement.
-
Spinal cord (short segment lesions) involvement in 20-30% of cases
-
Follow-up imaging:
- resolution or significant improvement of lesions
- Development of new lesions are atypical as classically a monophasic process
- If new lesions continue to develop, then other demyelinating conditions should be considered
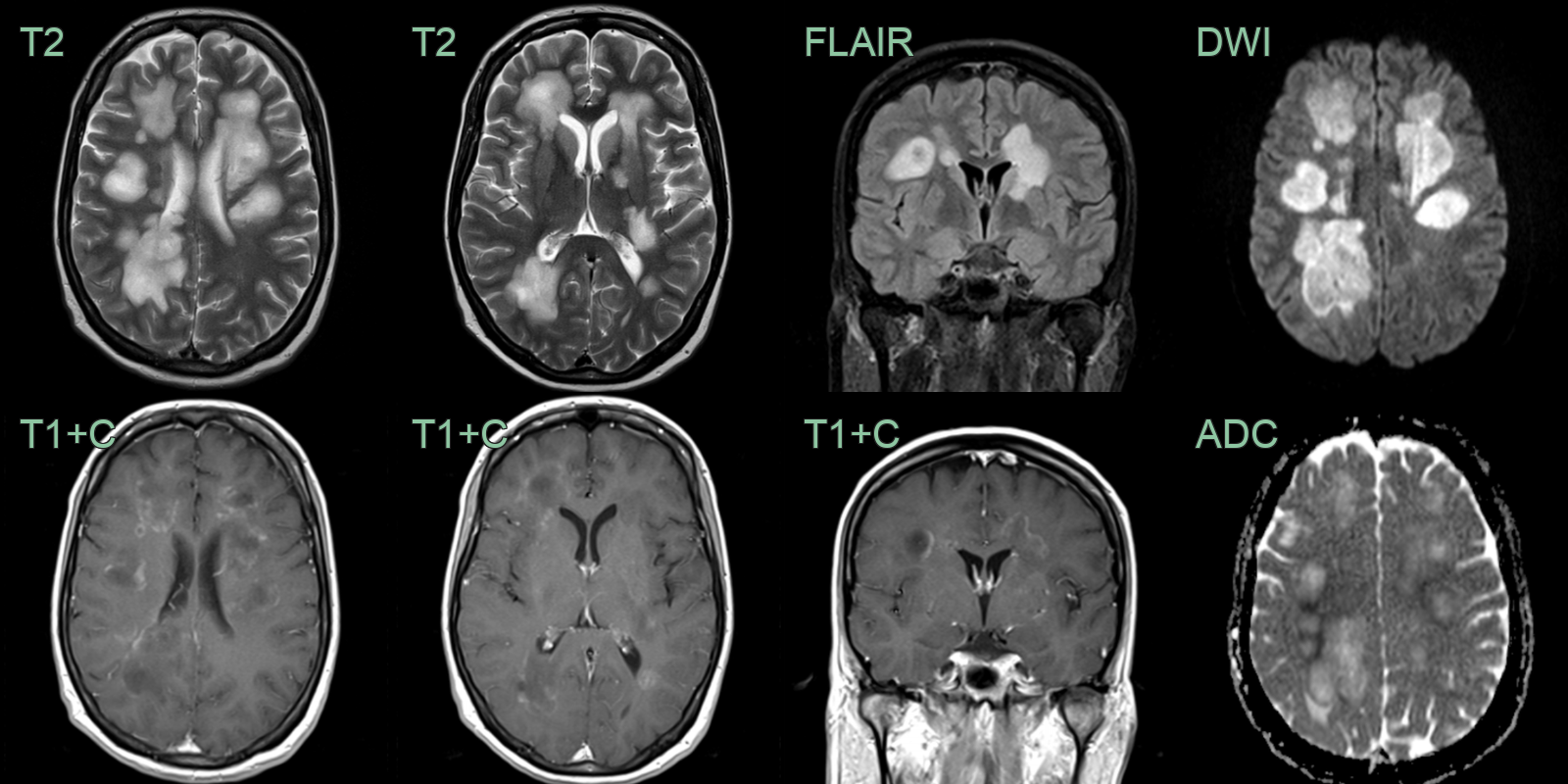
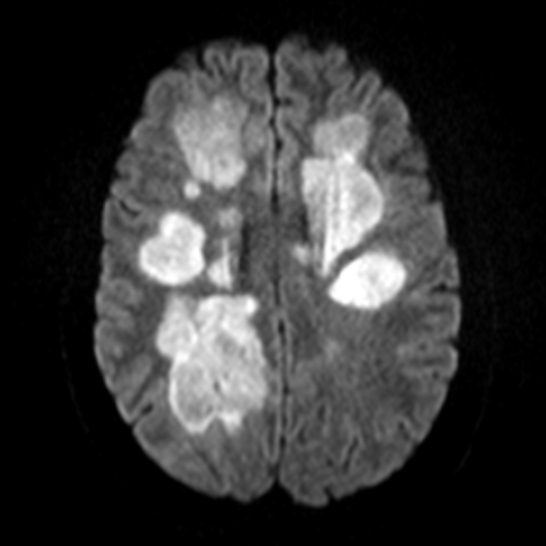
- One month after a viral upper respiratory tract infection, a 25-year-old patient presented with confusion and left sided weakness.
- MRI showed multifocal white matter lesions with incomplete rim enhancement.
- Some of the lesions had a leading edge of diffusion restriction.
Treatment¶
- High-dose IV corticosteroids first-line; IVIG or plasma exchange for refractory cases
- Usually monophasic with a good prognosis
Differential diagnosis¶
| Differential Diagnosis | Distinguishing Feature |
|---|---|
| Multiple Sclerosis | Ovoid periventricular plaques with Dawson's fingers on sagittal FLAIR; calloso-septal interface lesions; no basal ganglia involvement typical for MS |
| Acute Haemorrhagic Leukoencephalitis (AHLE) | Haemorrhagic foci on GRE/SWI within T2 lesions; more confluent white matter involvement; mass effect |
| Neuromyelitis Optica | Longitudinally extensive spinal cord lesion (>3 vertebral segments); bilateral optic nerve enhancement; area postrema involvement |
| Posterior Reversible Encephalopathy Syndrome | Posterior-predominant parieto-occipital vasogenic oedema with elevated ADC; no basal ganglia or brainstem involvement typical of PRES |
-
Pohl et al. Acute disseminated encephalomyelitis: Updates on an inflammatory CNS syndrome. 2016. Neurology - Open in new tab. ↩