Alzheimer's Disease¶
Summary

- Progressive neurodegenerative disorder characterised by cognitive decline and memory loss
- Pathologically defined by accumulation of amyloid plaques and neurofibrillary tangles
- Imaging shows cortical atrophy, particularly in medial temporal lobes and hippocampi1
Pathophysiology¶
- Accumulation of extracellular β-amyloid plaques
- Formation of intracellular neurofibrillary tangles composed of hyperphosphorylated tau protein
- Neuronal loss and synaptic dysfunction
- Neurotransmitter imbalances, particularly in cholinergic system
Demographics¶
- Most common cause of dementia, accounting for 60-80% of cases
- Prevalence increases with age:
- 3% in 65-74 year olds
- 17% in 75-84 year olds
- 32% in those 85 years and older
- Higher incidence in females
- Risk factors include:
- Advanced age
- Family history
- Apolipoprotein E ε4 allele
- Cardiovascular risk factors
- Lower educational attainment
Diagnosis¶
- Clinical assessment:
- Detailed history and cognitive evaluation
- Neurological examination
- Neuropsychological testing
- Exclusion of other causes of cognitive decline
- Biomarkers:
- Cerebral atrophy on imaging (see below)
- Cerebrospinal fluid (CSF) analysis for β-amyloid and tau proteins
- Genetic testing in familial cases
Imaging¶
- Structural imaging (MRI or CT):
- Disproportionate atrophy of hippocampi, mesial temporal lobes and the parietal lobes
- Enlarged ventricles due to subcortical volume loss
- Perfusion weighted imaging (e.g., ASL):
- Decreased CBF in parietal and temporal lobes
- Functional imaging:
- FDG-PET: reduced glucose metabolism in temporoparietal regions
- SPECT: reduced perfusion in temporoparietal regions
- Molecular imaging:
- Amyloid PET: increased cortical tracer uptake with loss of grey–white differentiation
- Tau PET: uptake tracks disease stage, spreading from mesial temporal to neocortical regions
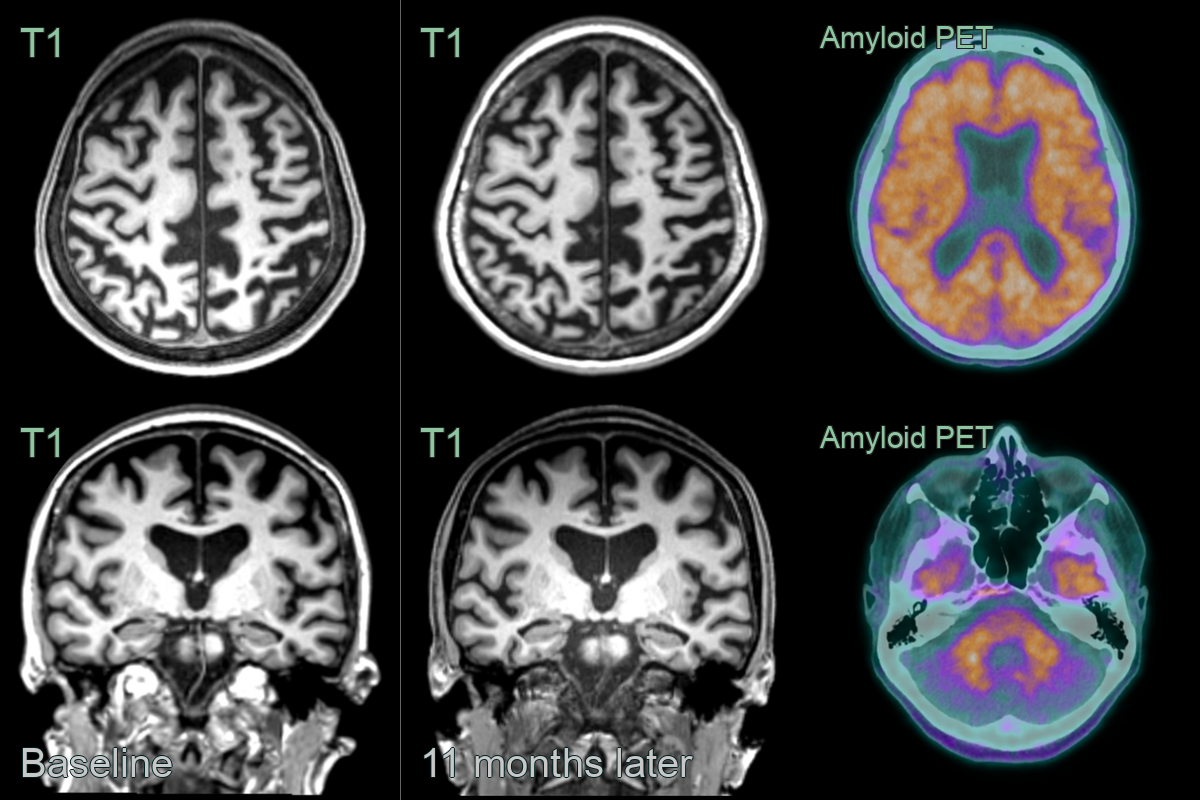
- 60-year-old patient presented with memory impairement. There was parietal and hippocampal (MTAS 2) volume loss. While the reduction in volume between the two scan was minimal, it was significant for such a short interval.
- Amyloid PET was postive with loss of supratentorial grey-white differentiation.
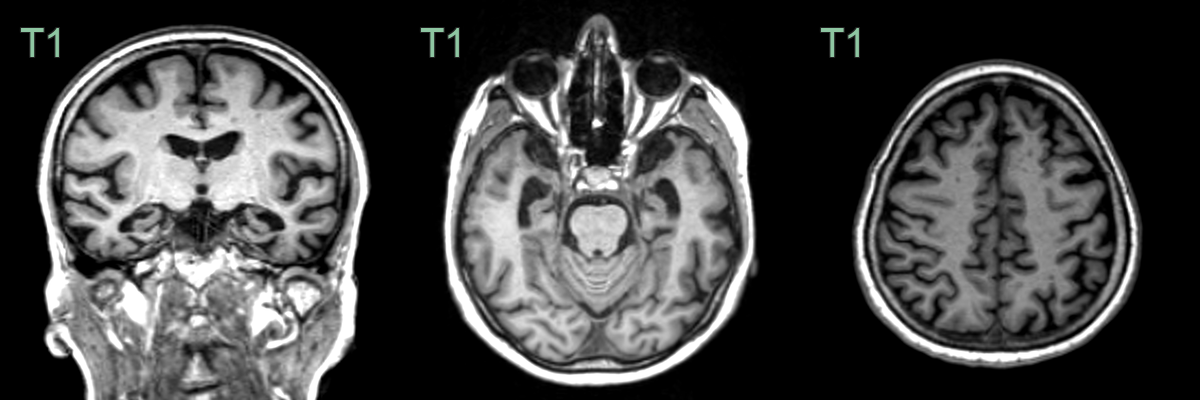
- 55-year-old patient with amnestic cognitive impairment.
- There was marked mesial and anterior temporal volume loss (MTAS 3).
- Parietal volume loss on the left was mild.
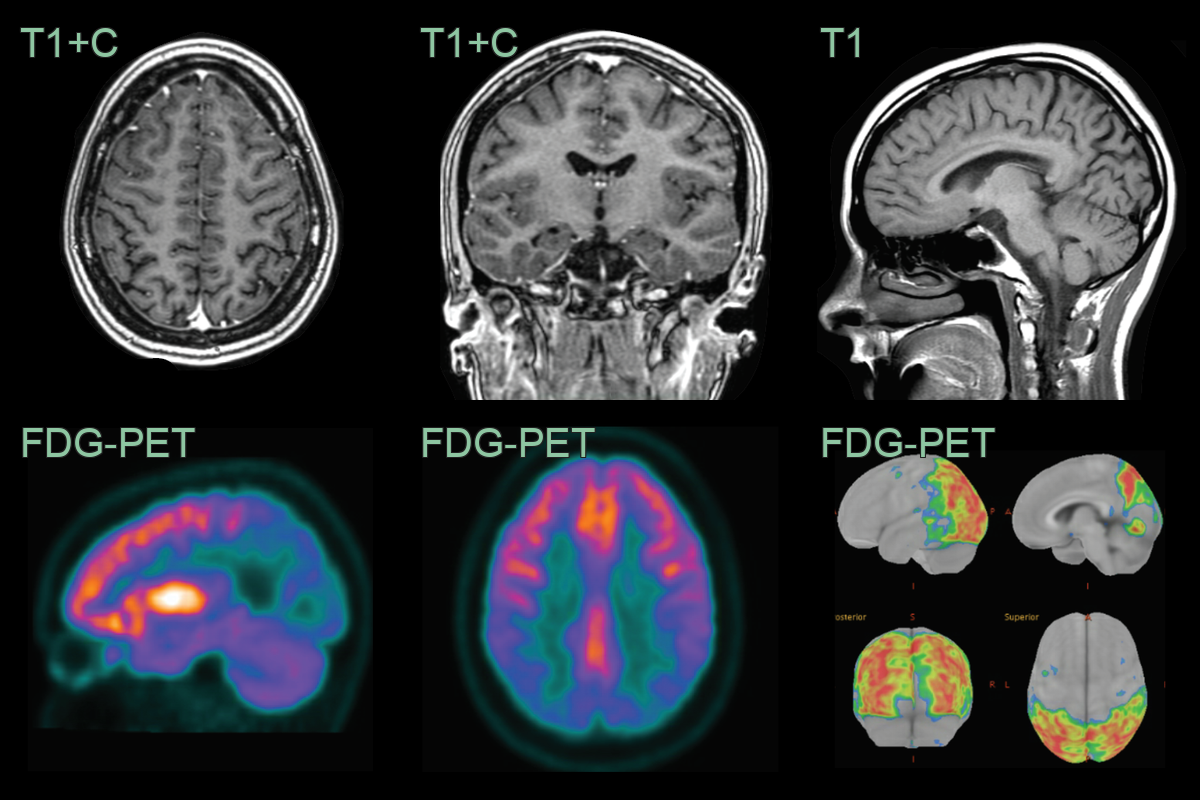
- A 30-year-old patient with a family history of Alzheimer's disease presented with cognitive impairment.
- While clearly abnormal for age, the volume loss in the parietal lobes was relatively mild. Hippocampal volume was within normal limits.
- FDG-PET showed marked hypometabolism in the parietal and occipital lobes. The Z-scores on standarised surface projection (Minoshima) maps were between -11 and -13.
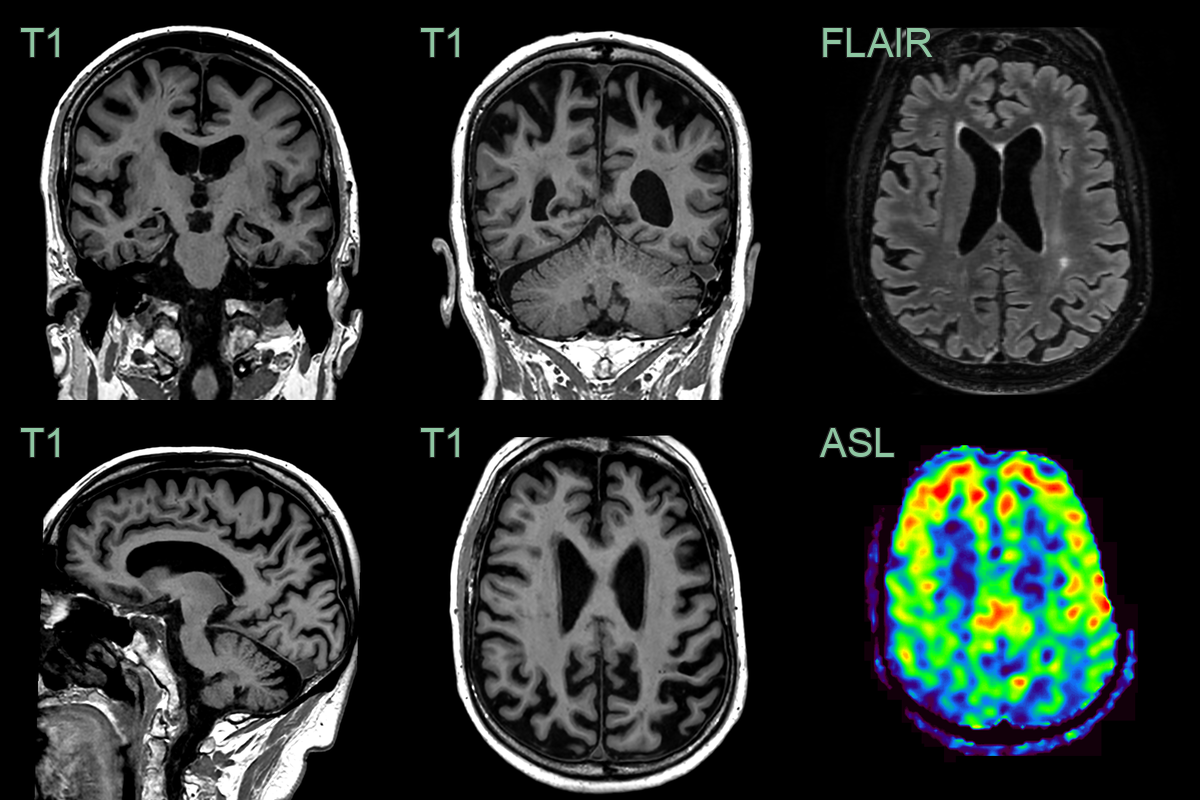
- A 75-year-old patient presented with memory impairment.
- MRI showed excessive volume loss affecting the hippocampi (MTAS 2.5-3) and parietal lobes.
- The parietal volume loss was paired with reduced CBF on ASL.
Treatment¶
- Pharmacological:
- Acetylcholinesterase inhibitors (donepezil, rivastigmine, galantamine)
- NMDA receptor antagonist (memantine)
- Management of behavioural and psychological symptoms
- Supportive care and caregiver education
- Emerging therapies:
- Immunotherapies aimed at amyloid and tau clearance
Differential diagnosis¶
| Imaging differential | Differentiating feature |
|---|---|
| Frontotemporal dementia | Frontal and/or anterior temporal-predominant atrophy, often asymmetric, with relative parietal sparing |
| Posterior cortical atrophy | Focal parieto-occipital atrophy with relatively spared hippocampi |
| Normal pressure hydrocephalus | Ventriculomegaly disproportionate to sulcal atrophy; tight high convexity and widened Sylvian fissures |
| Vascular dementia | Strategic infarcts and confluent white matter small-vessel disease |
| Dementia with Lewy bodies | Relatively preserved medial temporal volume despite dementia |
-
Scheltens et al. Alzheimer's disease. 2021. Lancet (London, England) - Open in new tab. ↩