Ankylosing Spondylitis¶
Summary
- Chronic inflammatory arthritis primarily affecting the axial skeleton
- Characterised by sacroiliitis, spinal fusion, and enthesitis
- Imaging shows bamboo spine appearance and syndesmophytes on radiographs1
Pathophysiology¶
- Autoimmune disorder with strong genetic association (HLA-B27)
- Chronic inflammation of the spine and sacroiliac joints
- Progressive ossification of ligaments and joint capsules
- Enthesitis at sites of ligament and tendon attachment
Demographics¶
- Typically affects young adults (20-40 years old)
- Male predominance (2-3:1 male to female ratio)
- Prevalence: 0.1-1.4% of general population
- Higher prevalence in HLA-B27 positive individuals
Diagnosis¶
- Clinical criteria: chronic back pain, morning stiffness, limited spinal mobility
- Laboratory findings: elevated ESR, CRP, and HLA-B27 positivity
- Imaging findings: sacroiliitis, syndesmophytes, bamboo spine
- ASAS (Assessment of SpondyloArthritis international Society) criteria
Imaging¶
Radiographs¶
- Sacroiliitis: erosions, sclerosis, and joint space narrowing
- Syndesmophytes: bony outgrowths bridging vertebral bodies
- Bamboo spine: complete fusion of vertebral bodies
- Squaring of vertebral bodies
- Enthesitis: whiskering at sites of ligament attachment
MRI¶
- Early detection of active inflammation
- Bone marrow oedema in sacroiliac joints and vertebral corners
- Fat metaplasia in chronic stages
- Erosions and sclerosis in advanced disease
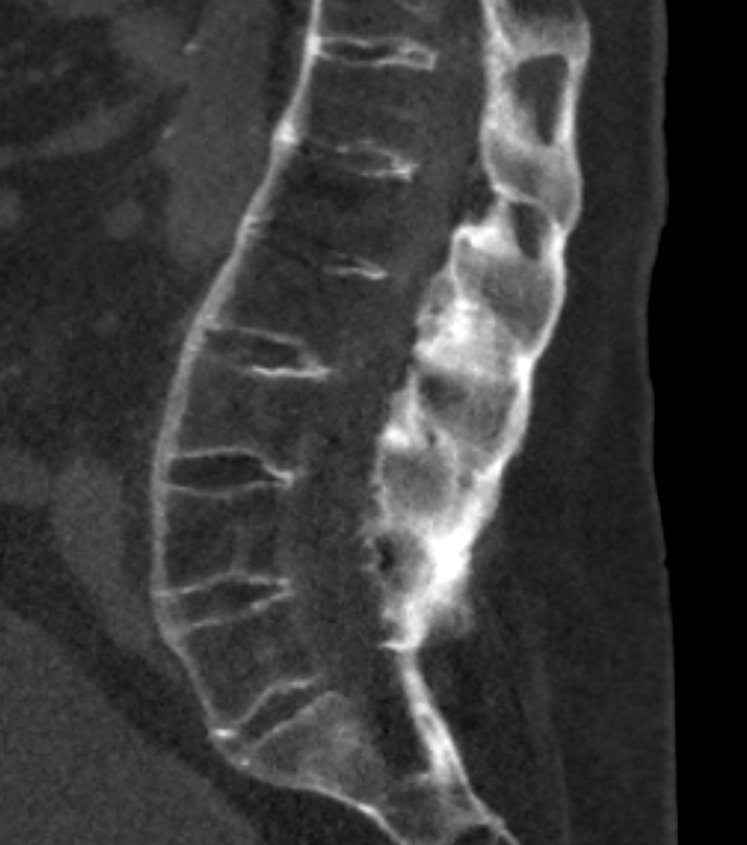
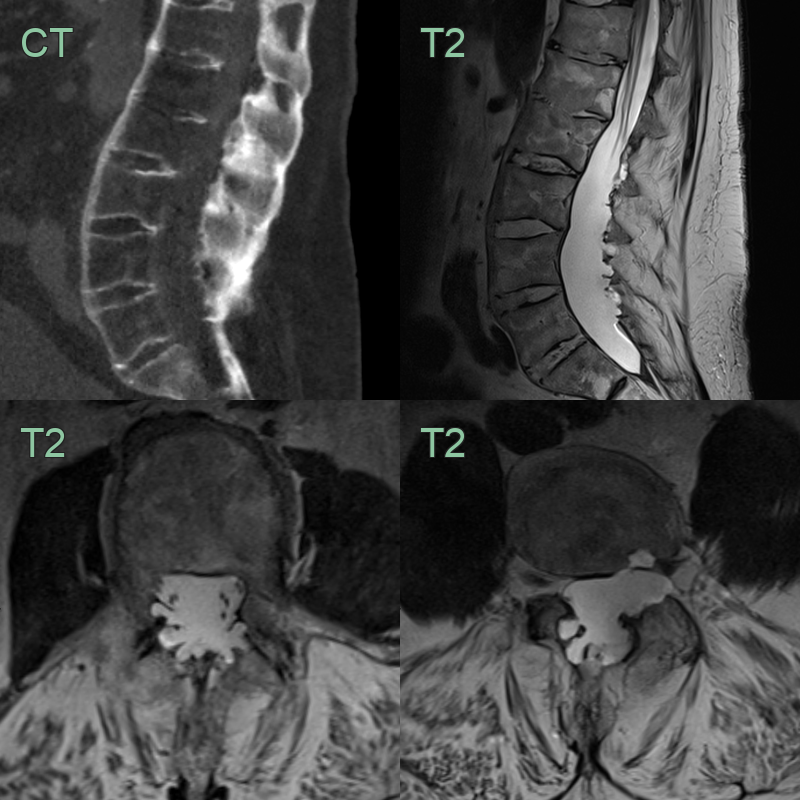
CT¶
- Best for syndesmophytes, ankylosis and fractures
Neuroradiological complications¶
- The rigid, ankylosed ("bamboo") spine behaves as a long bone: even minor trauma causes highly unstable, often transdiscal three-column fractures (carrot-stick fractures), typically in the lower cervical spine, with a high risk of epidural haematoma and cord injury — CT with a low threshold for MRI is mandatory
- Andersson lesion: a mobile pseudarthrosis through a fracture or non-fused segment
- Cauda equina syndrome with dorsal dural ectasia and arachnoid diverticula scalloping the posterior elements is a late complication
Treatment¶
- NSAIDs first-line; TNF or IL-17 inhibitors for active disease
- Surgical stabilisation for unstable fractures or progressive deformity
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Diffuse idiopathic skeletal hyperostosis (DISH) | Affects older population; no sacroiliitis; flowing ossification of anterior longitudinal ligament |
| Psoriatic arthritis | Presence of psoriasis; asymmetric sacroiliitis; more peripheral joint involvement |
| Reactive arthritis | Asymmetric sacroiliitis; peripheral asymmetric arthritis; no syndesmophytes |
| Enteropathic arthritis | May have asymmetric sacroiliitis without bamboo spine; sacroiliac joint asymmetry |
| Scheuermann's disease | Thoracic kyphosis with anterior vertebral body wedging; no sacroiliitis; no syndesmophytes |
-
Braun et al. Ankylosing spondylitis. 2007. Lancet (London, England) - Open in new tab. ↩