Bell's Palsy¶
Summary
- Acute, unilateral facial nerve paralysis of unknown etiology
- Characterised by sudden onset of facial weakness, typically affecting one side of the face
- Diagnosis primarily clinical, with imaging used to rule out other causes1
Pathophysiology¶
- Exact cause unknown, but believed to involve inflammation of the facial nerve (CN VII)
- Possible triggers include:
- Viral infections (e.g., herpes simplex virus, varicella-zoster virus)
- Immune-mediated processes
- Vascular ischaemia
- Inflammation leads to compression and oedema of the facial nerve within the facial canal
Demographics¶
- Annual incidence: 15-30 cases per 100,000 population
- Affects all age groups, but peak incidence in 15-45 years
- Slightly higher prevalence in:
- Pregnant women
- Patients with diabetes mellitus
- Individuals with upper respiratory tract infections
Diagnosis¶
- Primarily clinical, based on:
- Sudden onset of unilateral facial weakness
- Inability to close eye or wrinkle forehead on affected side
- Drooping of corner of mouth
- Physical examination:
- House-Brackmann scale to grade facial nerve function
- Assessment of taste and lacrimation
- Exclusion of other causes (e.g., stroke, tumour) through history and examination
Imaging¶
- Not routinely required for diagnosis
- May be used to rule out other causes or in cases of atypical presentation
- Modalities:
- MRI:
- T1-weighted with gadolinium: enhancement of the facial nerve
- FLAIR: hyperintensity of the facial nerve
- CT:
- Limited role in acute setting
- May show bony erosion in chronic cases
- Findings:
- Enhancement and swelling of the facial nerve, particularly in the labyrinthine and tympanic segments
- Normal brain parenchyma
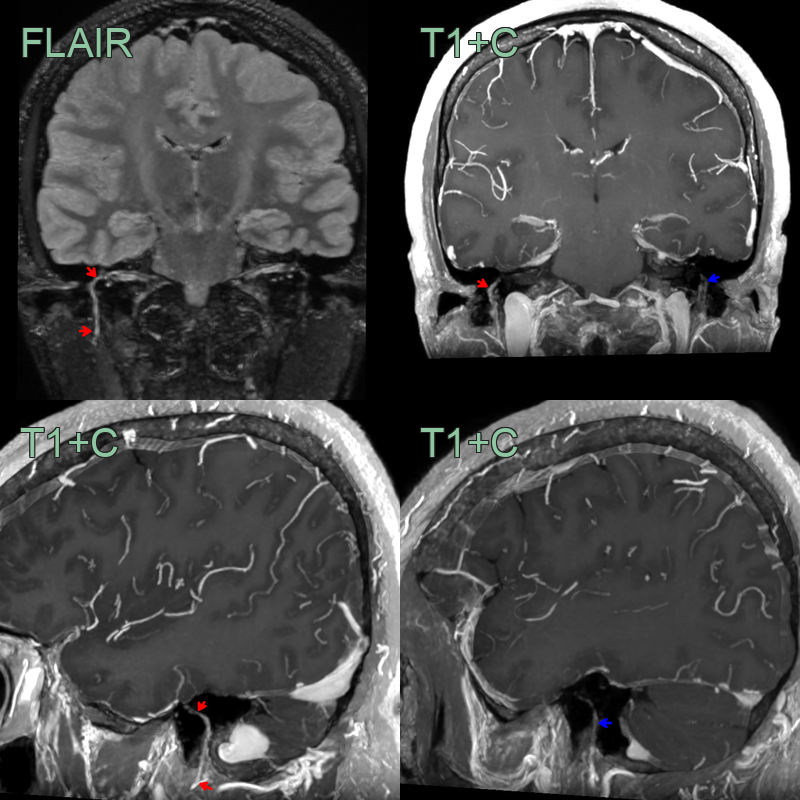
- 50-year-old patient presented with right sided facial weakness affecting the forehead.
- MRI showed a FLAIR hyperintensity, mild thickening, and pathological enhancement (labyrinthine, tympanic and mastoid segments; red arrow) of the right facial nerve and a normal left facial nerve (blue arrow).
Treatment¶
- Early corticosteroids (± antiviral) and eye protection
- Most recover completely within 3–6 months
Differential diagnosis¶
| Imaging differential | Differentiating feature |
|---|---|
| Ramsay Hunt syndrome | Enhancement of CN VII and VIII in the internal auditory canal, often with labyrinthine enhancement |
| Facial schwannoma | Focal enhancing, expansile mass along the nerve rather than smooth linear enhancement |
| Perineural tumour spread (parotid malignancy) | Thickened enhancing CN VII extending from a parotid/stylomastoid mass, widening the stylomastoid foramen |
| Leptomeningeal disease | Additional cranial nerve/pial enhancement |
Mild geniculate and tympanic-segment enhancement can be normal; asymmetric labyrinthine, canalicular or fundal enhancement suggests pathology.
-
Zhang et al. The etiology of Bell's palsy: a review. 2020. Journal of neurology - Open in new tab. ↩