Cerebral Amyloid Angiopathy-Related Inflammation (CAA-ri)¶
Summary
- CAA-ri is a rare inflammatory variant of cerebral amyloid angiopathy
- Characterised by acute to subacute onset of headache, cognitive decline, seizures, and focal neurological deficits
- MRI typically shows asymmetric white matter hyperintensities, microbleeds, and leptomeningeal enhancement1
Pathophysiology¶
- Inflammatory response to β-amyloid deposits in cerebral vessel walls
- Two proposed mechanisms:
- Autoimmune response against amyloid-β
- Excessive clearance of amyloid-β by activated microglia
- Associated with APOE ε4/ε4 genotype
Demographics¶
- Rare condition, exact prevalence unknown
- Typically affects older adults (mean age 67 years)
- No clear gender predilection
Diagnosis¶
- Clinical presentation:
- Acute to subacute onset of symptoms
- Headache, cognitive decline, seizures, focal neurological deficits
- Diagnostic criteria (all required) :
- Acute/subacute onset of symptoms
- Age ≥40 years
- ≥1 of: headache, decreased consciousness, behavioural change, focal neurological signs
- MRI findings consistent with CAA-ri
- Absence of neoplastic, infectious, or other cause
Imaging¶
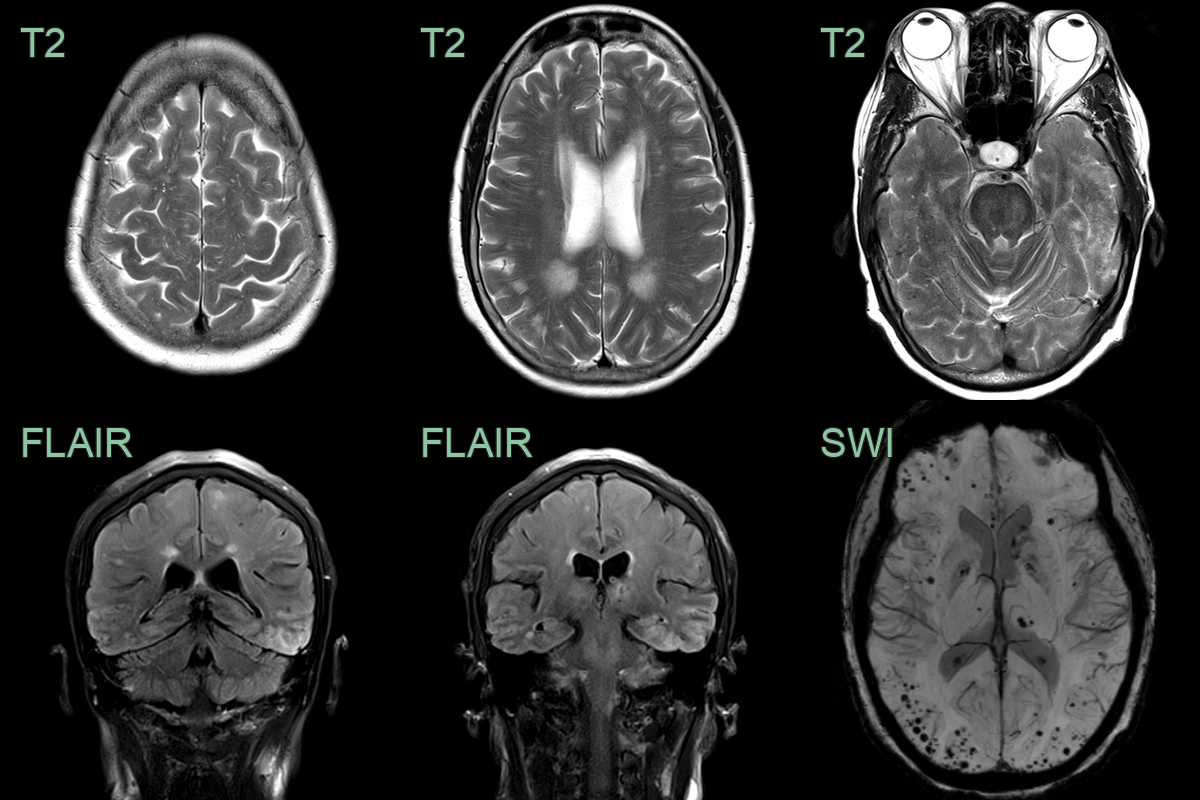
- MRI findings:
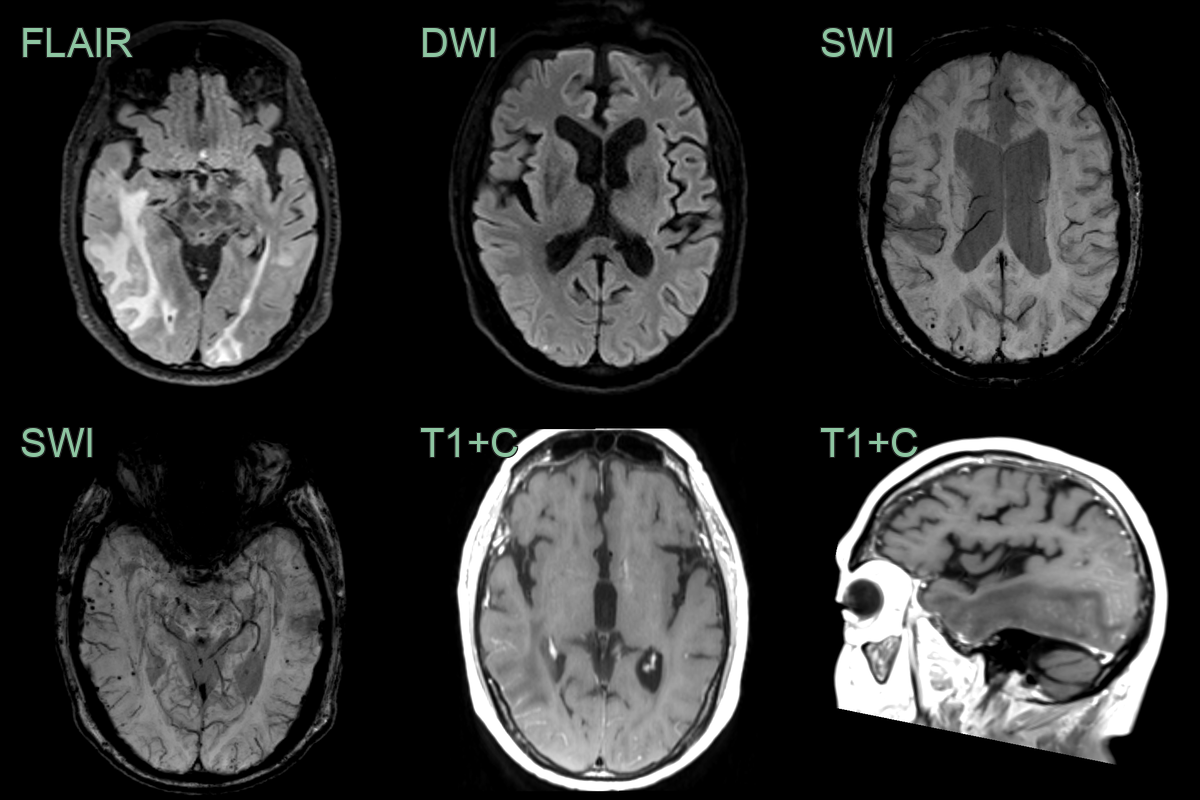
- Asymmetric white matter hyperintensities on T2/FLAIR
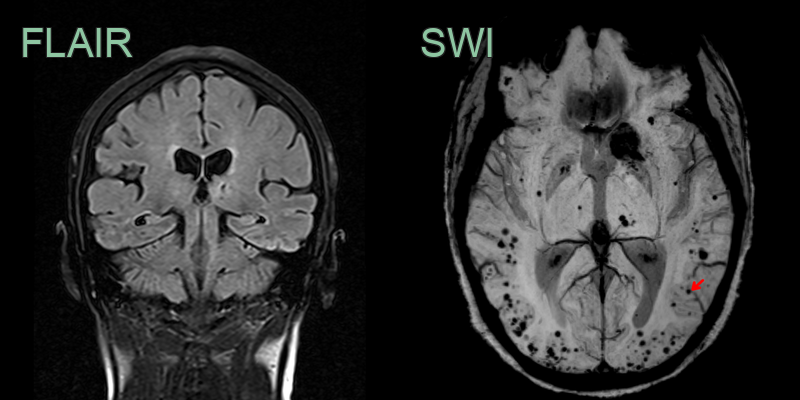
- Microbleeds on susceptibility-weighted imaging (SWI)
- Cortical superficial siderosis
- Leptomeningeal enhancement
- Lobar microbleeds or lobar haemorrhages
- CT findings:
- Hypodensities in affected white matter
- May show lobar haemorrhages
Treatment¶
- Immunosuppression (high-dose corticosteroids, occasionally cyclophosphamide) usually produces clinical and radiological improvement, supporting the diagnosis
Differential diagnosis¶
The key is the background of lobar microbleeds and cortical superficial siderosis; without it, consider:
| Imaging differential | Differentiating feature |
|---|---|
| PRES | Posterior-predominant vasogenic oedema, symmetric, resolves on follow-up, without lobar microbleeds/siderosis |
| Primary CNS vasculitis | Multifocal infarcts and vessel wall enhancement rather than confluent asymmetric white matter oedema |
| Infiltrating glioma | Expansile T2 signal with mass effect, no siderosis |
| Progressive multifocal leukoencephalopathy | Subcortical U-fibre disease with a restricting active edge, no enhancement or microbleeds |
-
Laterza et al. Cerebral amyloid angiopathy-related inflammation (CAA-ri): an updated systematic review and meta-analysis. 2026. Journal of neurology - Open in new tab. ↩