Epidural Haematoma¶
Summary
- Acute accumulation of blood between the dura mater and inner table of the skull
- Typically caused by arterial bleeding, often from the middle meningeal artery
- Classically presents with a "lucid interval" followed by rapid neurological deterioration1
Pathophysiology¶
- Arterial bleeding, usually from middle meningeal artery rupture
- Less commonly caused by venous bleeding from dural sinuses
- Blood accumulates between dura and skull, causing increased intracranial pressure
- Rapid expansion due to arterial pressure can lead to brain herniation
Demographics¶
- Most common in young adults and adolescents (20-30 years old)
- More frequent in males (3:1 male to female ratio)
- Often associated with traumatic brain injury, especially temporal bone fractures
- Rare in elderly due to increased dural adherence to skull
Diagnosis¶
- Clinical presentation:
- Initial loss of consciousness, followed by a lucid interval
- Rapid neurological deterioration
- Ipsilateral pupillary dilation
- Contralateral hemiparesis
- Glasgow Coma Scale assessment
- Neurological examination
- Immediate neuroimaging (CT or MRI)
Imaging¶
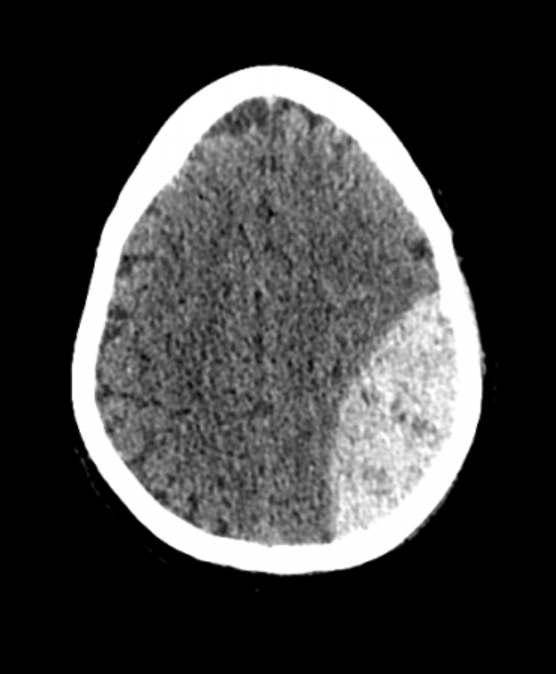
- CT scan (non-contrast):
- Hyperdense, biconvex (lenticular) extra-axial collection
- Does not cross suture lines
- May show associated skull fracture
- "Swirl sign" in active bleeding
- MRI:
- T1: isointense to brain in acute phase, hyperintense in subacute phase
- T2: heterogeneous signal intensity
- Susceptibility-weighted imaging (SWI): useful for detecting small haematomas
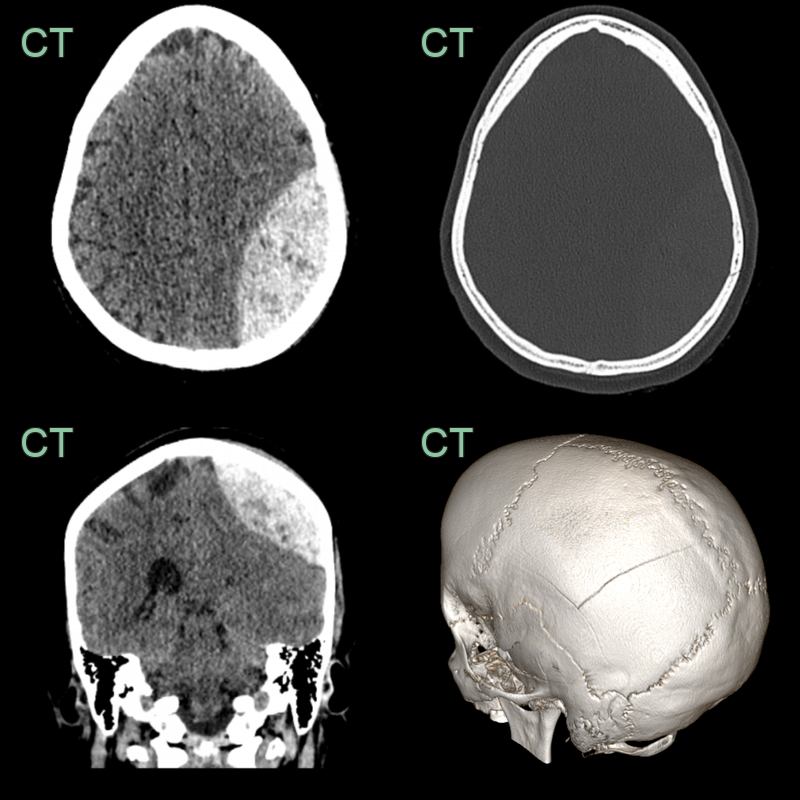
- 60-year-old patient presented after a head injury sustained after falling down a flight of stairs.
- CT showed a lentiform hyperdensity deep to a parietal bone fracture.
Treatment¶
- Emergent neurosurgical evaluation
- Surgical evacuation for:
- Haematoma volume > 30 mL
- Midline shift > 5 mm
- Thickness > 15 mm
- Burr hole or craniotomy depending on size and location
- Conservative management for small, asymptomatic haematomas:
- Close neurological monitoring
- Serial imaging
- Osmotic diuretics to control intracranial pressure
- Prognosis generally good with prompt diagnosis and treatment
Differential diagnosis¶
| Imaging differential | Differentiating feature |
|---|---|
| Subdural haematoma | Crescentic and crosses sutures but not the midline; epidural is biconvex and bounded by sutures |
| Epidural empyema | Rim-enhancing collection with restricted diffusion; infective context rather than acute trauma |
| Dural-based tumour (e.g. meningioma) | Enhancing soft-tissue mass, not hyperdense clot; no fracture |
-
Berker et al. Traumatic epidural haematoma of the posterior fossa in childhood: 16 new cases and a review of the literature. 2003. British journal of neurosurgery - Open in new tab. ↩