Fibromuscular Dysplasia (FMD)¶
Summary
- Fibromuscular dysplasia is a non-inflammatory, non-atherosclerotic arteriopathy affecting medium-sized arteries
- Characterised by abnormal cellular growth in arterial walls, leading to stenosis, aneurysm, or dissection
- Most commonly affecting the renal and cerebrovascular arteries to cause a typical 'string of beads' appearance on angiography1
Pathophysiology¶
- Exact aetiology unknown, likely multifactorial
- Involves fibrous tissue overgrowth in arterial walls, leading to:
- Intimal fibroplasia
- Medial fibroplasia (most common)
- Perimedial fibroplasia
- Adventitial fibroplasia
- Results in arterial stenosis, aneurysm formation, or dissection
Demographics¶
- Predominantly affects females (9:1 female to male ratio)
- Typically diagnosed between ages 30-50
- More common in Caucasians
- Prevalence estimated at 3-4% in general population
Diagnosis¶
- Often asymptomatic and discovered incidentally
- Clinical presentation depends on affected arteries:
- Cerebrovascular FMD: headache, pulsatile tinnitus, stroke
- Renal FMD: hypertension, flank pain, renal infarction
- Mesenteric FMD: abdominal pain, weight loss
- Diagnosis confirmed with angiography
Imaging¶
- CTA / MRA / DSA:
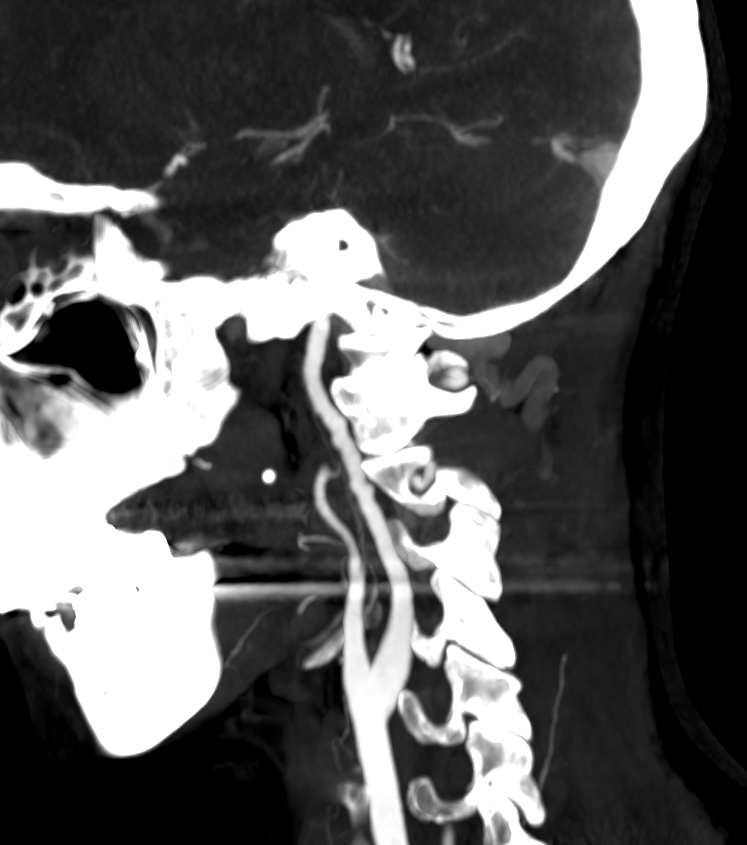
- Medial fibroplasia (most common) gives the classic "string of beads" — alternating stenoses and dilatations — in the mid and distal cervical ICA and vertebral arteries, characteristically sparing the origin (unlike atherosclerosis)
- Intimal fibroplasia produces a smooth long-segment stenosis, web or tubular narrowing
- Screen for associated dissection, aneurysm (including intracranial) and renal artery disease
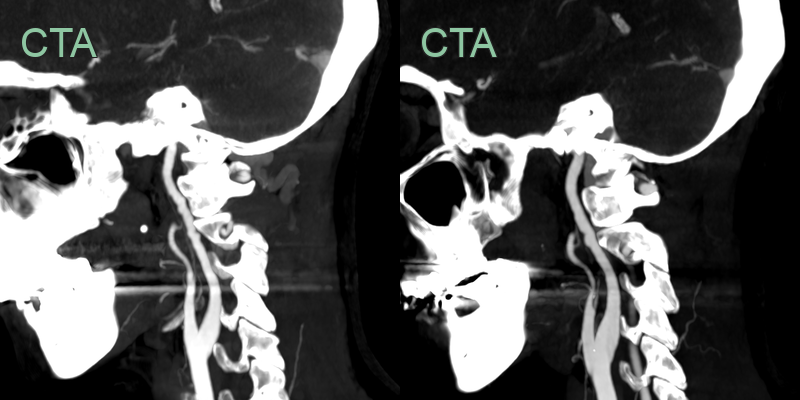
- A CTA was performed in an adult female patient with vertigo.
- The corrugated contour of the cervical ICAs was compatible with FMD.
- There was no acute infarct on the MRI and there was no history of renal dysfunction.
Treatment¶
- Antiplatelet therapy and blood-pressure control; angioplasty for flow-limiting stenosis or dissection
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Atherosclerosis | FMD typically affects younger patients and lacks traditional cardiovascular risk factors |
| Carotid artery dissection | Can co-exist and can be difficult to differentiate. Dissection typically causes mural T1-hyperintensity and usually occures at proximal ICA of just below skull base, less likely to cause long segment luminal irregularity that is seen in FMD |
| Vasculitis | Vasculitis typically causes smooth, tapered luminal narrowing with vessel wall thickening and mural enhancement, often affects multiple vascular territories, and may be associated with systemic inflammatory markers, unlike the "string of beads" appearance of FMD |
-
Slovut et al. Fibromuscular dysplasia. 2004. The New England journal of medicine - Open in new tab. ↩