Fungal Sinusitis¶
Summary
- Fungal sinusitis is an infection of the paranasal sinuses caused by various fungal species
- Clinical presentation ranges from indolent to rapidly progressive, depending on the type and host immune status
- Imaging findings vary but often include sinus opacification and characteristic hyperdense foci on CT1
Pathophysiology¶
- Two main categories: non-invasive and invasive forms
- Non-invasive:
- Fungal ball (mycetoma)
- Allergic fungal sinusitis (AFS)
- Invasive:
- Acute invasive fungal sinusitis
- Chronic invasive fungal sinusitis
- Granulomatous invasive fungal sinusitis
- Common causative fungi:
- Aspergillus species
- Mucorales (e.g., Rhizopus, Mucor)
- Dematiaceous fungi (e.g., Bipolaris, Curvularia)
Demographics¶
- Non-invasive forms:
- Fungal ball: more common in older adults, female predominance
- AFS: typically affects younger adults, history of atopy
- Invasive forms:
- Acute: immunocompromised patients (e.g., diabetics, transplant recipients)
- Chronic: immunocompetent individuals in endemic areas (e.g., Sudan, India)
- Granulomatous: immunocompetent individuals in tropical and subtropical regions
Diagnosis¶
- Clinical presentation:
- Non-invasive: chronic sinusitis symptoms, nasal polyps (in AFS)
- Invasive: fever, facial pain, orbital symptoms, neurological deficits
- Laboratory findings:
- Elevated serum IgE and eosinophilia in AFS
- Fungal cultures and histopathology
- Endoscopic examination:
- Visualisation of fungal debris or characteristic mucin
Imaging¶
- CT findings:
- Fungal ball:
- Focal hyperdense material within an opacified sinus
- Calcifications or metallic densities
- AFS:
- Expansile sinus opacification with hyperdense mucin
- "Double density" sign
- Bone remodelling and thinning
- Invasive forms:
- Aggressive bone destruction
- Soft tissue invasion
- Orbital and intracranial extension
- MRI findings:
- Fungal ball:
- T1 and T2 hypointense signal
- Peripheral enhancement
- AFS:
- Characteristically very low (even signal-void) T2 central mucin with a T2-hyperintense peripheral mucosal rim
- Invasive forms:
- Variable signal intensity
- Enhancement of invaded tissues
- Restricted diffusion in acute invasive fungal sinusitis
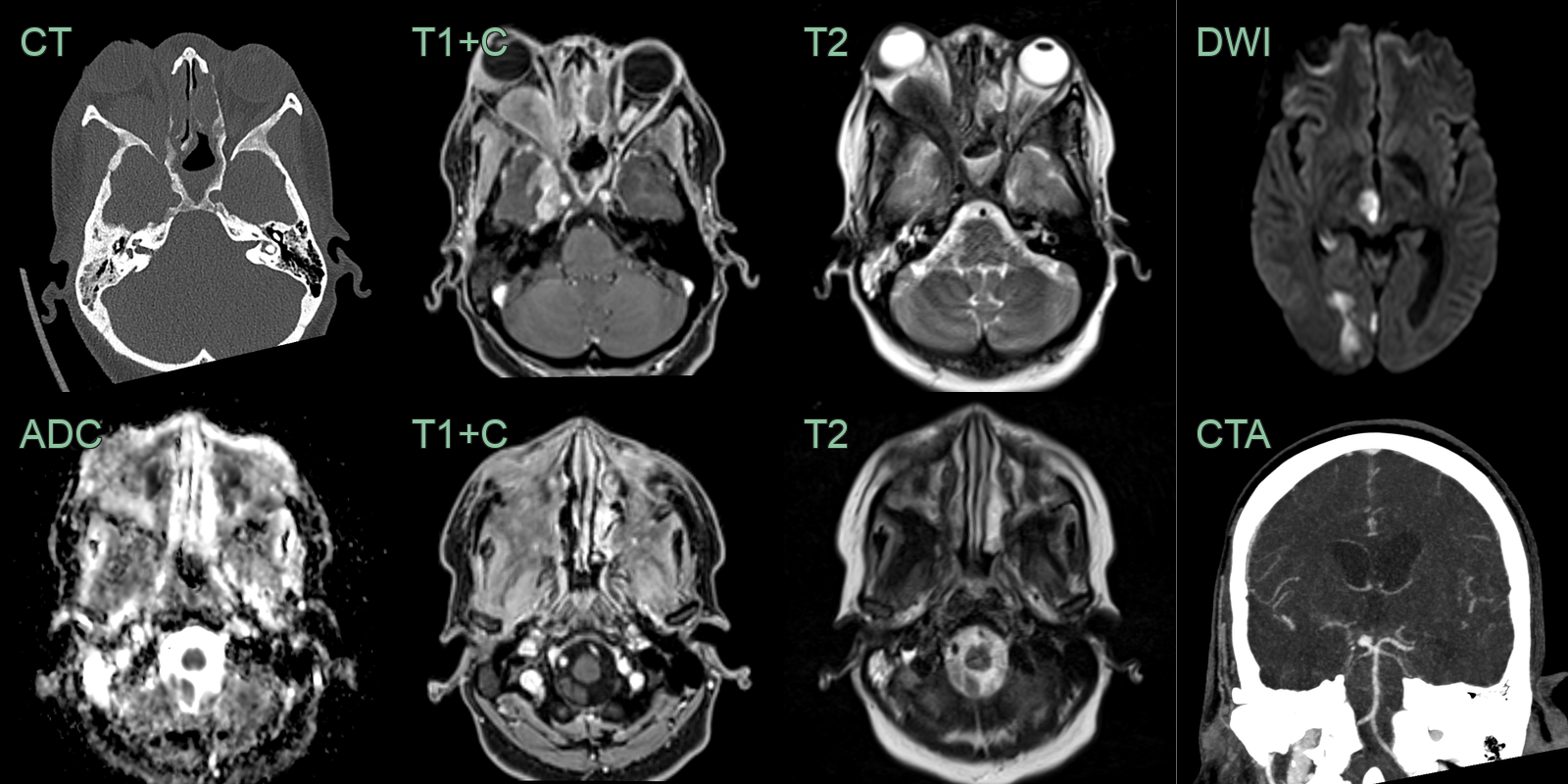
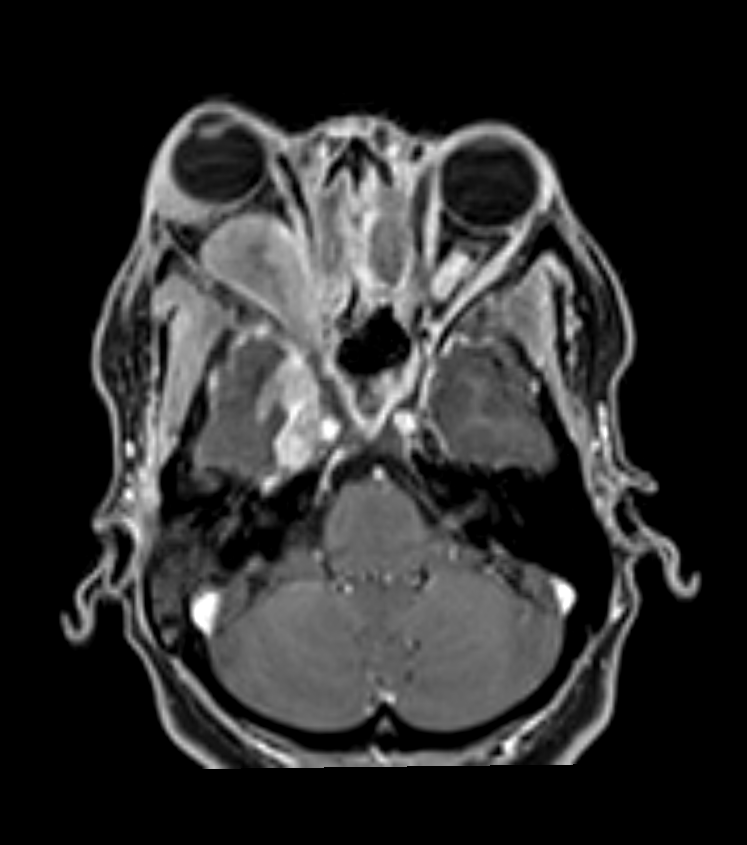
- A 50-year-old immunocompetent patient presented with right sided proptosis and headache.
- CT showed hyperostosis secondary to chronic sinusitis.
- MRI showed enhancing material filling the maxillary sinuses with regions of diffusion restriction.
- There was intracranial extension of T2-hypointense disease along the dura of the right middle cranial fossa and intraorbital extension.
- 2 weeks after admission and some clinical response to anti-fungal treatment, the patient developed a left visual field defect and left sided numbness. CTA and DWI showed a right PCA infarct due to an occlusion distal to a mycotic aneurysm.
Treatment¶
- Non-invasive disease: surgical removal ± steroids
- Acute invasive disease is an emergency: urgent debridement, systemic antifungals and reversal of immunosuppression
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Nasal Polyps | Smooth polypoid mucosal thickening without bone destruction or hyperdense fungal debris |
| Sinonasal Malignancy | Aggressive bone destruction and soft tissue mass with enhancement and diffusion restriction |
| Mucormycosis | Rapid progression with orbital/intracranial extension and devascularised "black turbinate" sign |
| Aspergilloma | Single sinus expansion with hyperdense concretions on CT and markedly low T2 signal |
| Inverted papilloma | Unilateral sinonasal mass with cerebriform T2 pattern and focal hyperostosis at stalk |
-
Raz et al. Fungal Sinusitis. 2015. Neuroimaging clinics of North America - Open in new tab. ↩