Herpes Simplex Virus (HSV) encephalitis¶
Summary
- Acute necrotizing encephalitis caused by HSV-1 or HSV-2
- Typically affects temporal and frontal lobes
- Characterised by fever, altered mental status, and focal neurological deficits1
Pathophysiology¶
- HSV-1 is the most common cause in adults (90% of cases)
- HSV-2 more common in neonates and immunocompromised individuals
- Virus enters via olfactory or trigeminal nerve pathways
- Causes cytotoxic and vasogenic oedema, haemorrhage, and necrosis
- Predilection for limbic structures, particularly temporal lobes
Demographics¶
- Incidence: 2-4 cases per million per year
- Bimodal age distribution:
- Peak in young adults (20-30 years)
- Second peak in older adults (>50 years)
- No gender predilection
- Can occur in all age groups, including neonates
Diagnosis¶
- Clinical presentation:
- Fever, headache, altered mental status
- Focal neurological deficits (e.g., aphasia, hemiparesis)
- Seizures (70% of cases)
- Laboratory findings:
- CSF analysis: pleocytosis, elevated protein, normal glucose
- PCR detection of HSV DNA in CSF (sensitivity >95%, specificity >99%)
- EEG: periodic lateralized epileptiform discharges (PLEDs)
Imaging¶
- CT findings:
- Early: normal or subtle low attenuation in affected areas
- Late: haemorrhage, contrast enhancement, mass effect
- MRI findings (more sensitive than CT):
- T2/FLAIR: hyperintense signal in affected regions
- DWI: restricted diffusion in acute phase
- T1 post-contrast: gyral enhancement
- SWI: petechial haemorrhages
- Typical distribution:
- Asymmetric involvement of temporal lobes (95% of cases)
- Frontal lobe involvement (80% of cases)
- Insular cortex, cingulate gyrus may be affected
- Sparing of basal ganglia
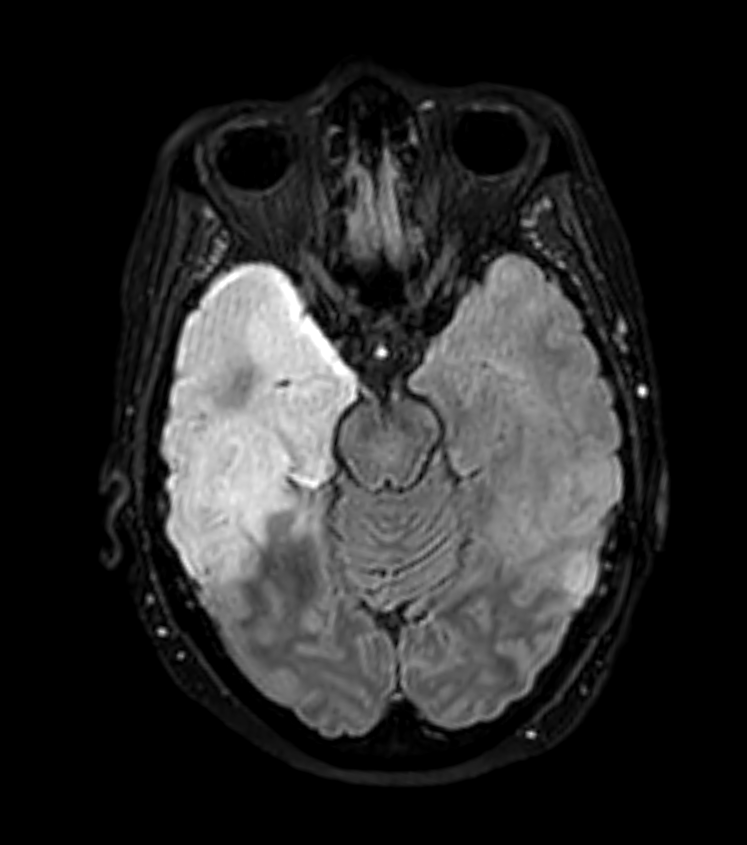
- 50-year-old patient presented with headache and confusion.
- CT showed swelling and low attenuation in the anterior and mesial left temporal lobe and in the right hippocampus.
- The parenchymal low attenuation gave the impression of a hyperdense vessel (Mach effect) but infarction was not likely as both MCA and PCA territories were involved.
- There was high T2, FLAIR and DWI signal (without clear diffusion restriction) but no enhancement.
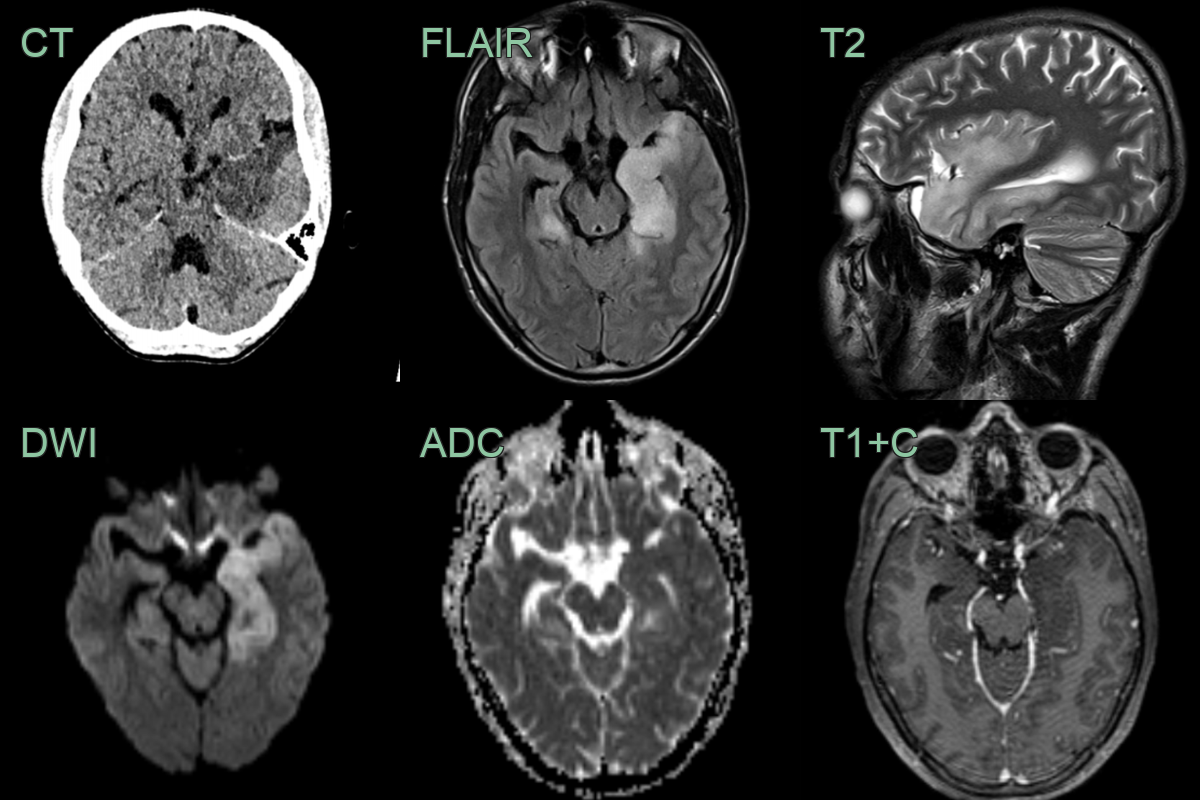
- 40-year-old patient presented with 2 day history of confusion and reduced GCS, headache and fever.
- MRI showed hyperintensity and swelling of the right mesial temporal lobe and diffusion restriction extending up to the right parietal lobe.
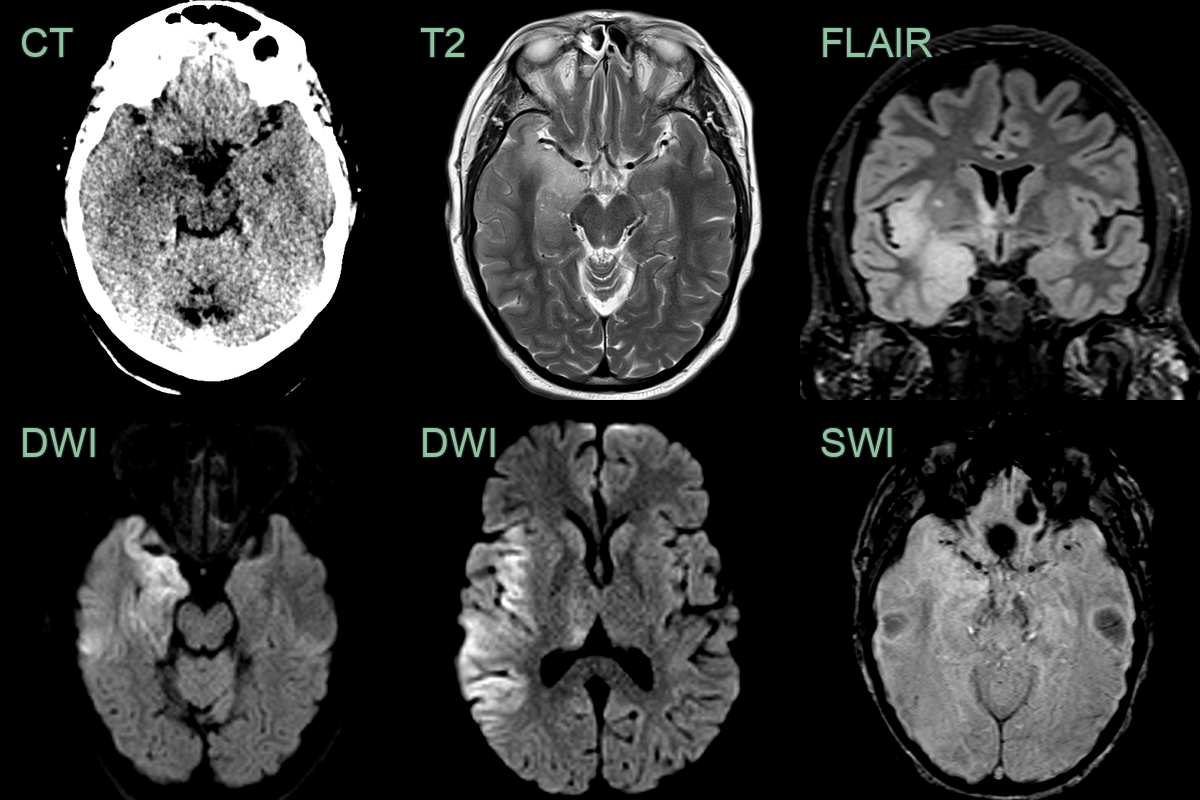
- 70-year-old patient presented with dysphasia and right-sided weakness and seizures. HSV was identified in CSF.
- MRI showed diffusion restriction in the cortex of left cerebral hemisphere as well as the right insula. There was swelling and subtle cortical enhancement.
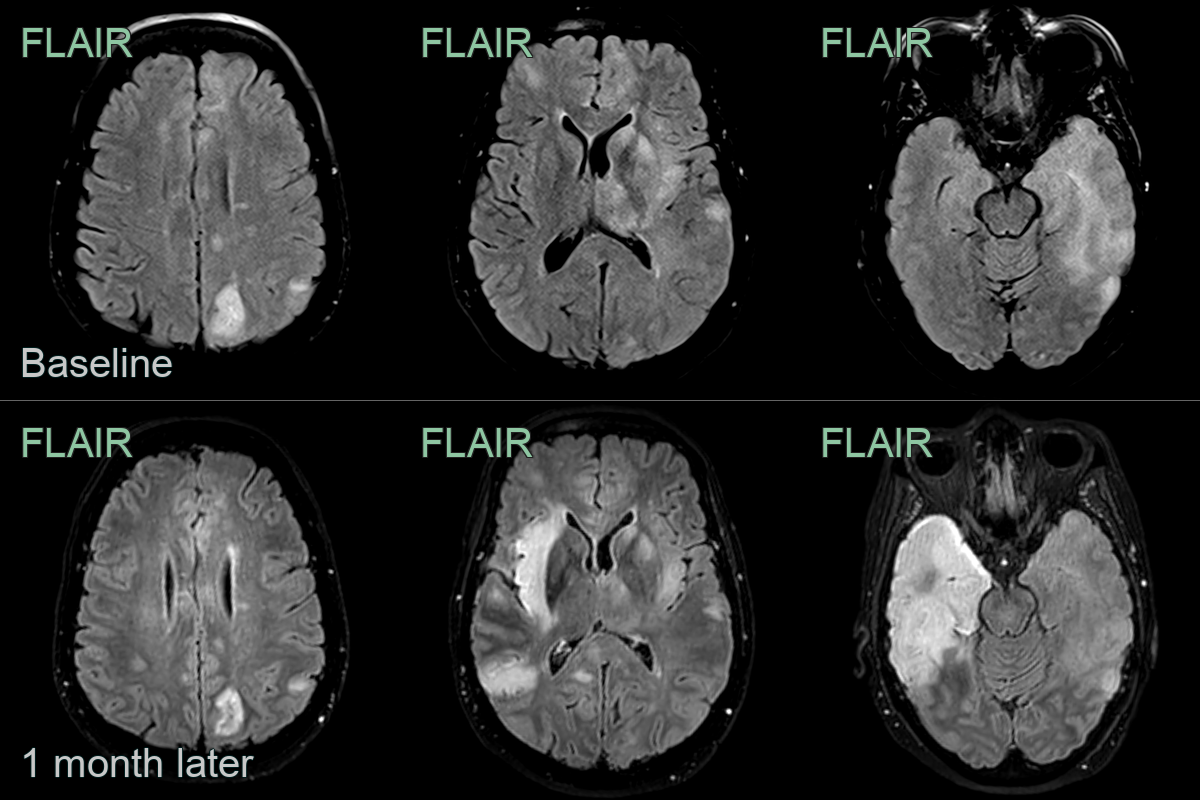
- 60-year-old patient presented with expressive dysphasia.
- MRI showed diffuse patchy cortical, white matter and ganglionic hyperintensity.
- On follow-up, hyperintensity involving most of the left temporal lobe resolved while marked hyperintensity developed in the right temporal lobe.
- Despite being repeatedly negative on CSF, brain biopsy revealed an HSV encephalitis.
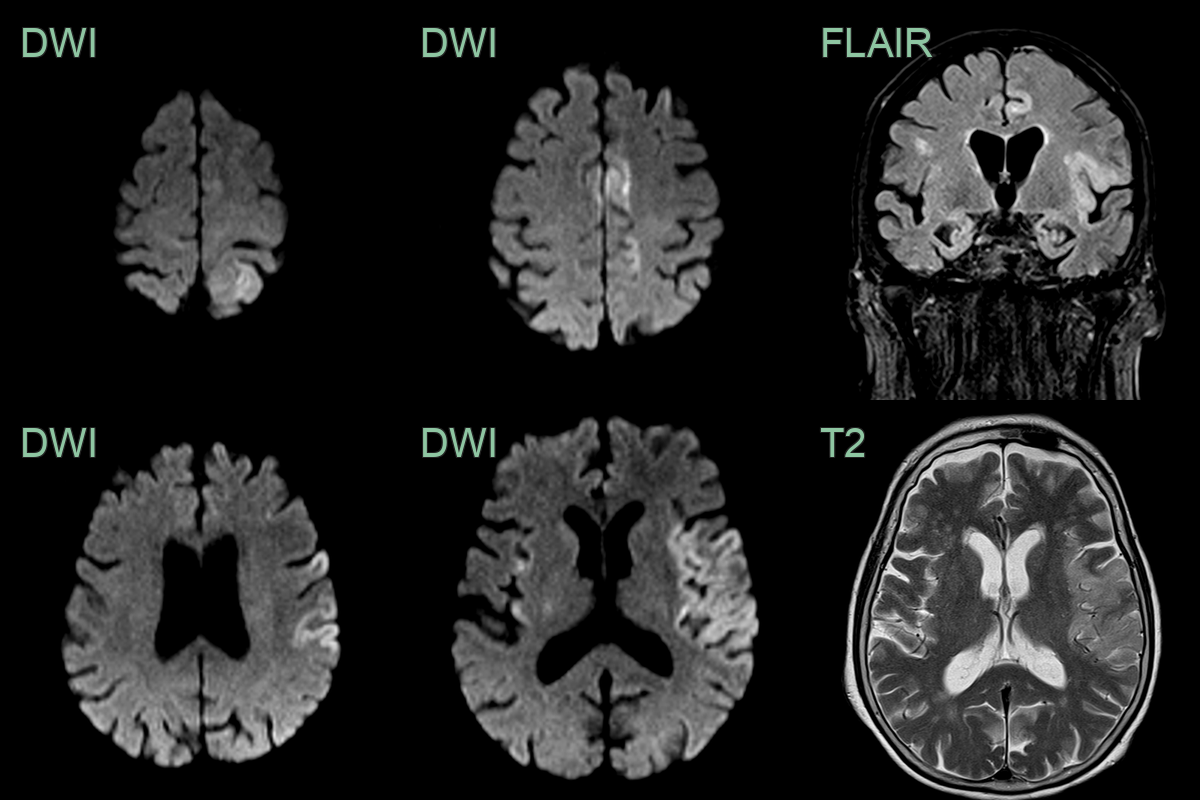
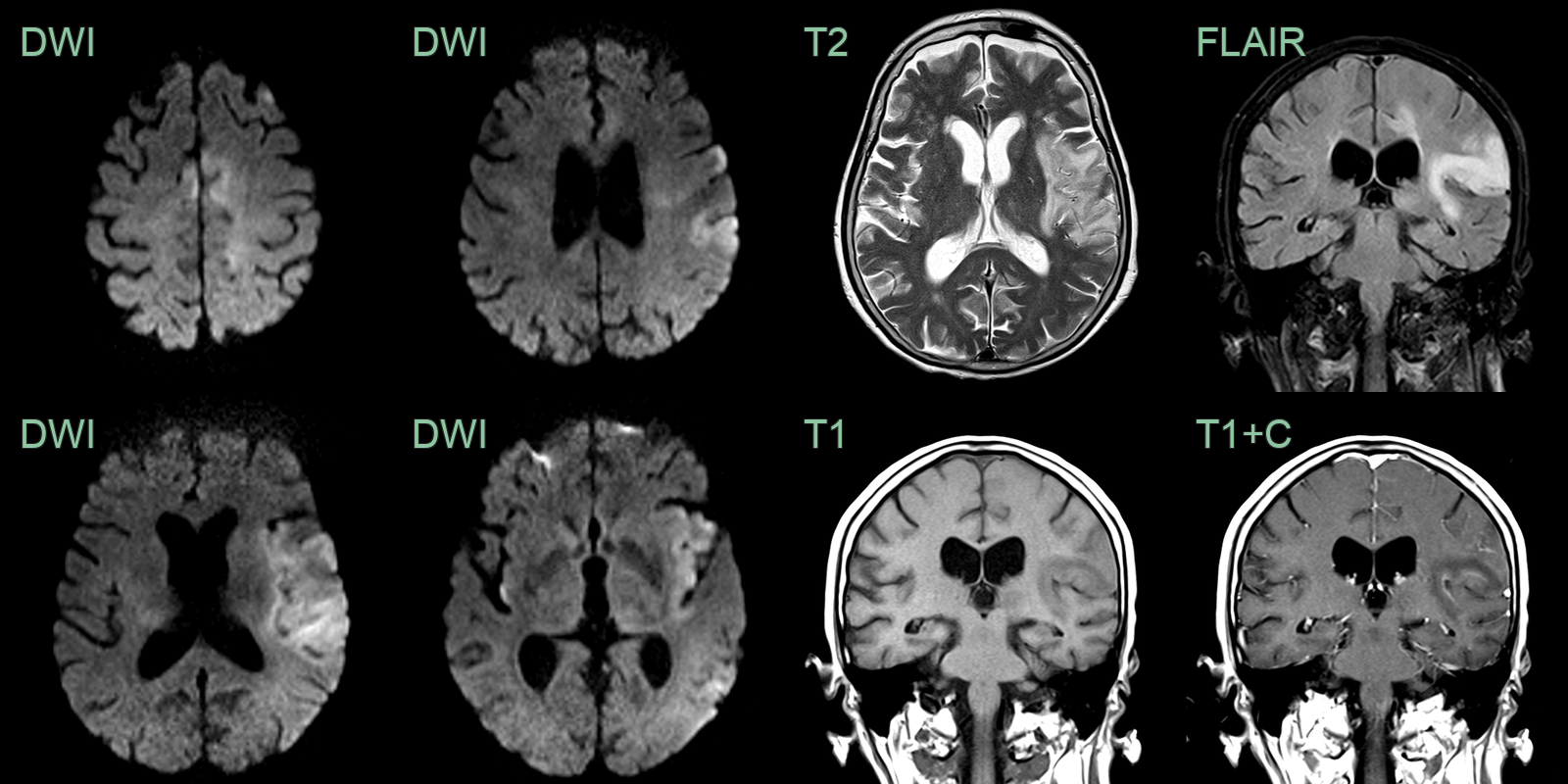
- 75-year-old patient presented with dysphasia and right sided weakness.
- MRI showed cortical DWI hyperintensity in the left frontal, parietal, temporal lobes and insular cortex bilaterally.
- Initially concerned about an acute infarct, the widespread and exclusively cortical involvement and a normal CTA, made HSV encephalitis more likely (which was confirmed on CSF analysis).
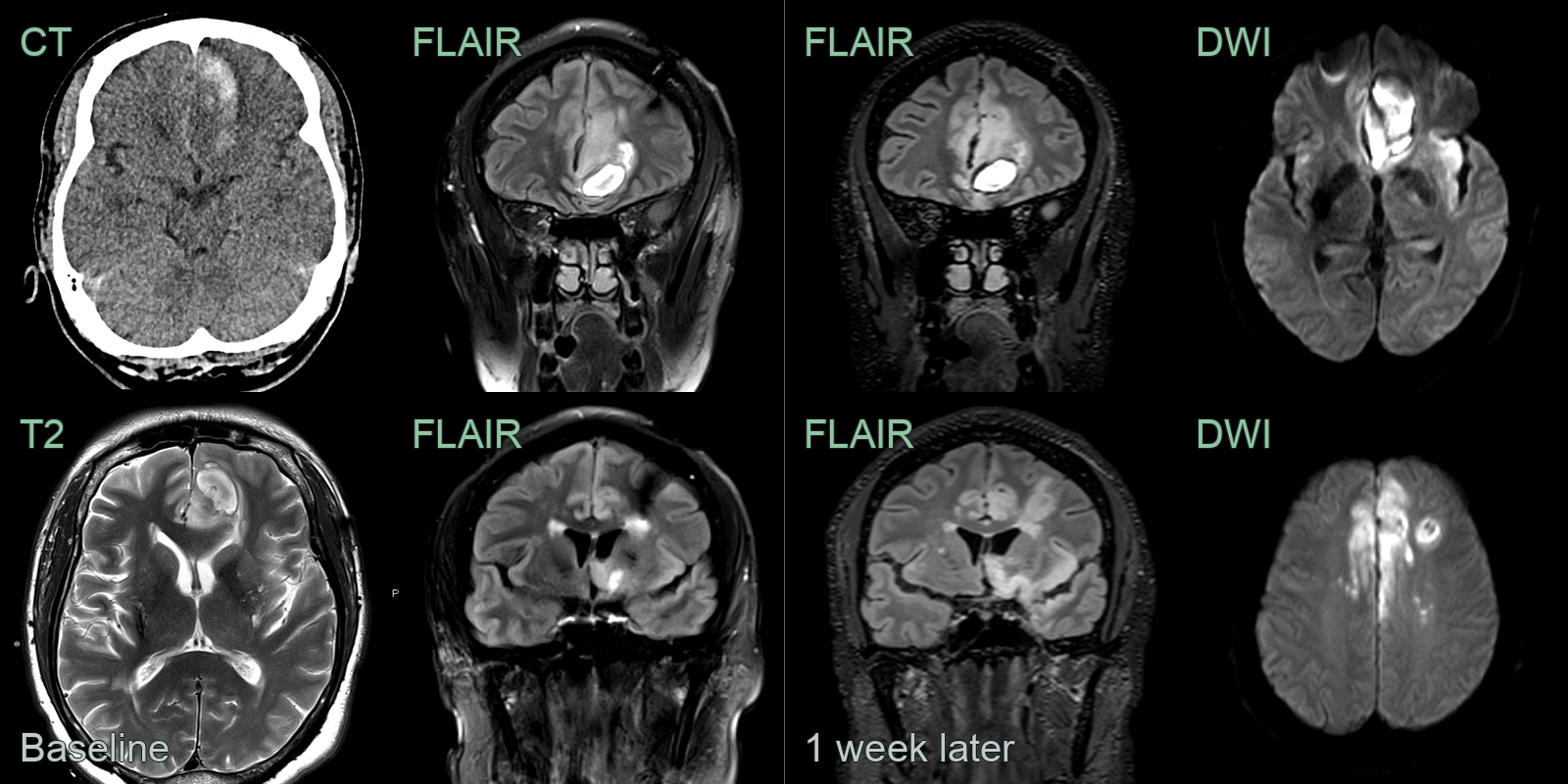
- A 45-year-old patient presented with right sided weakness and a fever.
- CT showed a haematoma in the left paramedian frontal lobe.
- MRI showed oedema around the haematoma as well as subtle high FLAIR signal in the cortex of the left frontal lobe and the right cingulate.
- On follow-up imaging, the FLAIR hyperintensity (and diffusion restriction) had extended through the limbic system.
- CSF HSV-1 PCR was positive.
Treatment¶
- Empirical IV aciclovir must be started on suspicion, before confirmation, as early treatment dramatically reduces mortality
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Autoimmune limbic encephalitis | Bilateral mesial temporal FLAIR hyperintensity without haemorrhage; typically no cortical ribboning on DWI; may enhance |
| MCA infarction | Confined to MCA vascular territory; involves basal ganglia; no involvement of contralateral mesial temporal lobe |
| Gliomatosis cerebri / low-grade glioma | Infiltrative T2 signal without swelling or DWI restriction; no cortical haemorrhage or gyral enhancement |
| Neurosyphilis | Mesiotemporal T2 hyperintensity similar to HSV; leptomeningeal and cortical enhancement; infarcts from vasculitis |
| Other viral encephalitides (HHV-6, VZV, EBV) | Similar mesiotemporal involvement; indistinguishable on imaging alone |
-
Si et al. Analysis of Metagenomic Next-Generation Sequencing (mNGS) in the Diagnosis of Herpes Simplex Virus (HSV) Encephalitis with Normal Cerebrospinal Fluid (CSF). 2023. Infection and drug resistance - Open in new tab. ↩