HTLV-1 associated myelopathy¶
Summary

- Chronic progressive myelopathy caused by human T-cell lymphotropic virus type 1 (HTLV-1)
- Characterised by spastic paraparesis, bladder dysfunction, and sensory disturbances
- MRI typically shows thoracic cord atrophy and T2 hyperintensities1
Pathophysiology¶
- HTLV-1 infects CD4+ T cells, leading to:
- Inflammatory response in the spinal cord
- Demyelination and axonal degeneration
- Cytokine-mediated damage to neurons and glial cells
- Genetic factors may influence susceptibility to developing myelopathy
Demographics¶
- Prevalence:
- Endemic in Japan, Caribbean, South America, and parts of Africa
- Estimated 5-10 million infected individuals worldwide
- Risk factors:
- Vertical transmission (mother to child)
- Sexual transmission
- Blood transfusion (rare in countries with blood screening)
- Age of onset: typically 30-50 years
- Female to male ratio: 2:1
Diagnosis¶
- Clinical presentation:
- Gradual onset of lower limb weakness and spasticity
- Bladder and bowel dysfunction
- Lower back pain and sensory disturbances
- Laboratory tests:
- HTLV-1 antibodies in serum and cerebrospinal fluid (CSF)
- PCR for HTLV-1 proviral DNA
- CSF analysis:
- Mild pleocytosis
- Elevated protein levels
- Oligoclonal bands (in some cases)
Imaging¶
- MRI findings:
- Thoracic cord atrophy (most common finding)
- T2 hyperintensities in the thoracic cord
- Symmetrical periventricular white matter lesions (in some cases)
- Spinal cord:
- Preferential involvement of lateral and posterior columns
- Minimal to no gadolinium enhancement
- Brain:
- Non-specific white matter lesions (in advanced cases)
- Cerebral atrophy (rare)
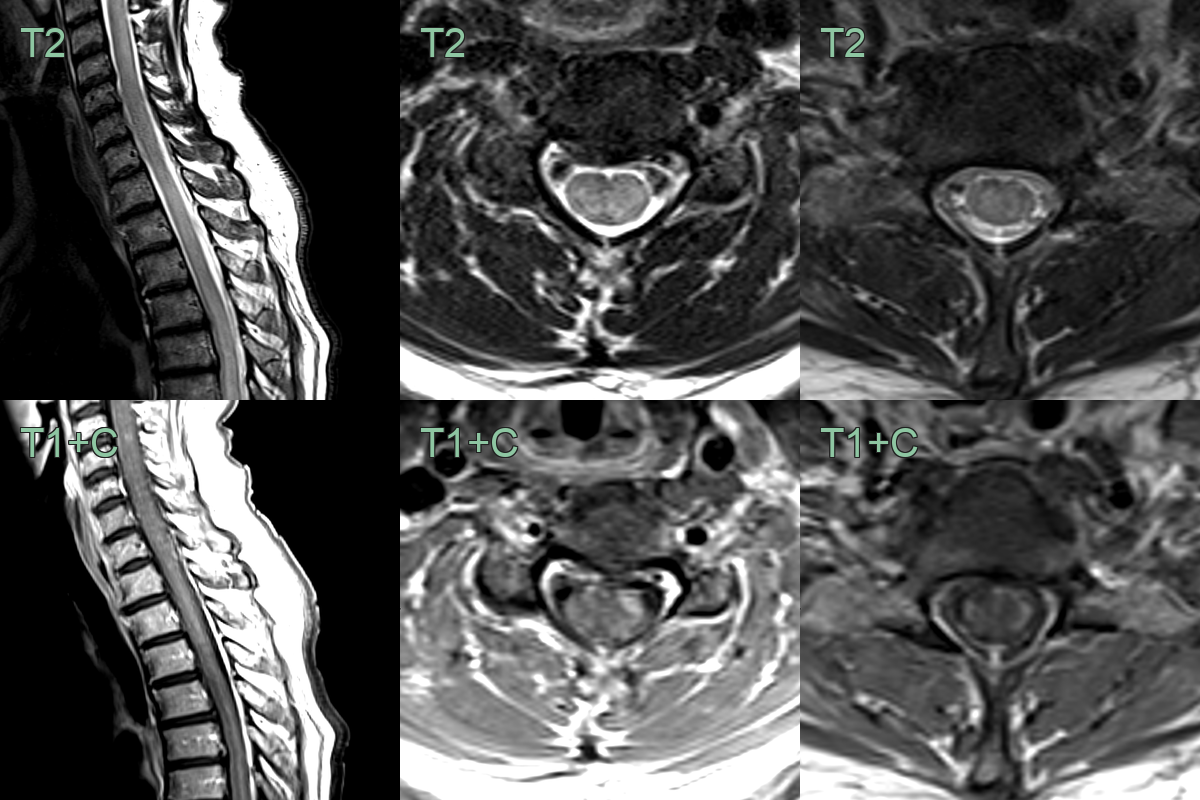
- 55-year-old patient presented with lower limb weakness, paraesthesia and areflexia.
- MRI showed a mildly swollen and hyperintense cervical and thoracic cord with patchy, mainly peripheral, enhancement.
- On follow-up imaging after 2 months, the hyperintensity persisted but the swelling and enhancement resolved.
Treatment¶
- No curative therapy; corticosteroids and symptomatic management. Diagnosis rests on HTLV-1 serology plus thoracic cord atrophy/T2 signal
Differential diagnosis¶
| Differential Diagnosis | Distinguishing Feature |
|---|---|
| Neuromyelitis Optica (NMO) | Longitudinally extensive T2 hyperintensity spanning ≥3 vertebral segments; central cord involvement; optic nerve lesions |
| Multiple Sclerosis | Short segment cord lesions (<2 vertebral segments); dorsolateral cord; periventricular and juxtacortical brain lesions |
| Transverse myelitis | Acute onset cord T2 hyperintensity with swelling; may enhance; can be indistinguishable in acute phase |
| HIV vacuolar myelopathy | Posterior and lateral column involvement; associated brain white matter changes |
| Subacute combined degeneration | Dorsal column T2 hyperintensity on axial MRI ("inverted V" sign); may involve posterior cervical and thoracic cord |
| Anterior spinal artery ischaemia | Anterior horn and corticospinal tract "owl-eye" or "snake-eye" pattern; diffusion restriction acutely |
| Hereditary spastic paraplegia | Cord atrophy; lateral column involvement; no acute inflammatory lesions |
-
Bangham et al. HTLV-1-associated myelopathy/tropical spastic paraparesis. 2015. Nature reviews. Disease primers - Open in new tab. ↩