IgG4-related disease¶
Summary
- Systemic fibroinflammatory condition characterised by elevated serum IgG4 levels and tissue infiltration by IgG4-positive plasma cells
- Affects multiple organs, commonly pancreas, salivary glands, and retroperitoneum
- Imaging findings include organ enlargement, mass-like lesions, and fibrosis1
Pathophysiology¶
- Exact aetiology unknown, likely autoimmune in nature
- Characterised by:
- Lymphoplasmacytic infiltration with IgG4-positive plasma cells
- Storiform fibrosis
- Obliterative phlebitis
- Elevated serum IgG4 levels (>135 mg/dL) in 60-70% of patients
- T helper 2 (Th2) and regulatory T (Treg) cell responses play a crucial role
Demographics¶
- Predominantly affects middle-aged to elderly males
- Male to female ratio approximately 3:1
- Peak incidence in the sixth and seventh decades of life
- Increasing recognition worldwide, but true prevalence unknown
Diagnosis¶
- Comprehensive diagnostic criteria include:
- Characteristic clinical features
- Elevated serum IgG4 levels
- Histopathological findings
- Organ-specific diagnostic criteria exist for some manifestations (e.g., autoimmune pancreatitis)
- Differential diagnosis includes malignancy, other autoimmune conditions, and infection
-
Tissue biopsy often required for definitive diagnosis
-
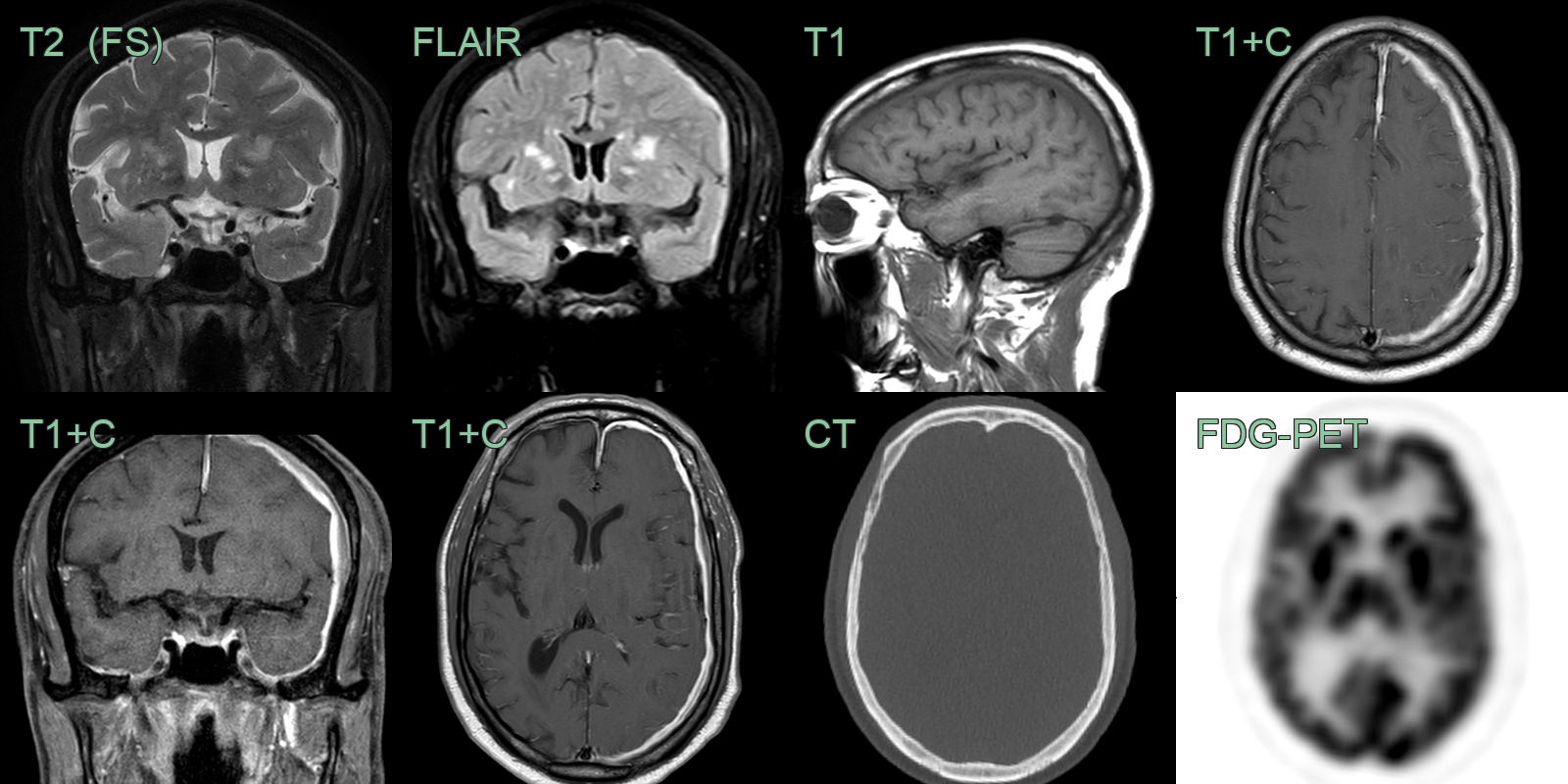
Head, neck and CNS manifestations relevant to neuroradiology:
- Hypertrophic pachymeningitis: focal or diffuse dural thickening and enhancement, T2-hypointense (fibrosis)
- Hypophysitis: thickened, enhancing pituitary stalk and gland, often with diabetes insipidus
- Orbital disease: enlarged lacrimal glands, infraorbital nerve and extraocular muscles; orbital "pseudotumour"
- Bilateral symmetrical salivary and lacrimal gland enlargement (Mikulicz disease); perineural spread along the trigeminal branches
- Systemic clues: "sausage-shaped" pancreas (autoimmune pancreatitis), biliary strictures and periaortic "coated aorta"
Treatment¶
- Corticosteroids first-line, with rituximab for relapsing or refractory disease; usually steroid-responsive
-
Perugino et al. IgG4-related disease: an update on pathophysiology and implications for clinical care. 2020. Nature reviews. Rheumatology - Open in new tab. ↩