Lipoma of the Corpus Callosum¶
Summary
- Congenital malformation from maldifferentiation of the meninx primitiva, not a neoplasm; usually incidental.
- Frequently associated with callosal dysgenesis; symptoms, when present, usually reflect the associated malformation rather than the lipoma.
- Midline pericallosal macroscopic fat, often calcified on CT, suppressing on fat-saturated MRI.
Pathophysiology¶
- Abnormal persistence and adipose differentiation of the meninx primitiva, the embryologic precursor of the leptomeninges and subarachnoid space 1
- Lies in the interhemispheric/pericallosal cistern; pericallosal arteries and, less often, neural tissue may run through it
- Strong association with agenesis or dysgenesis of the corpus callosum
- Two morphologic types 2
- Tubulonodular: bulky, anterior, often >2 cm and calcified; more often associated with callosal dysgenesis and other forebrain malformations
- Curvilinear: thin, posterior, follows the callosal margin; corpus callosum usually normal or only mildly dysgenetic
Demographics¶
- Rare; detected prenatally or incidentally at any age
- No sex predilection; most patients are asymptomatic
Diagnosis¶
- Usually an incidental imaging diagnosis; macroscopic fat is diagnostic and biopsy is unnecessary
- Reported associations include seizures, headache, and developmental delay — attribute symptoms to the associated malformation rather than the lipoma itself
Imaging¶
- Report: morphologic type and extent; corpus callosum formation; associated cortical malformation, interhemispheric cyst, or encephalocele; and the course of the pericallosal arteries through the lesion
- CT
- Homogeneous fat attenuation (approximately -50 to -100 HU)
- Peripheral or nodular calcification, especially in the tubulonodular type
- MRI
- T1: markedly hyperintense; sagittal imaging best shows the callosal relationship
- Fat suppression (fat-sat or Dixon): signal drops out, confirming macroscopic fat
- T2/FLAIR: hyperintense unless fat-suppressed
- Chemical-shift artifact at the fat–brain interface; no true diffusion restriction
- Post-contrast: no internal enhancement, though traversing vessels may enhance; noninfiltrative and should not cause edema
- Prenatal ultrasound: echogenic midline mass; fetal MRI better characterizes callosal development and associated anomalies
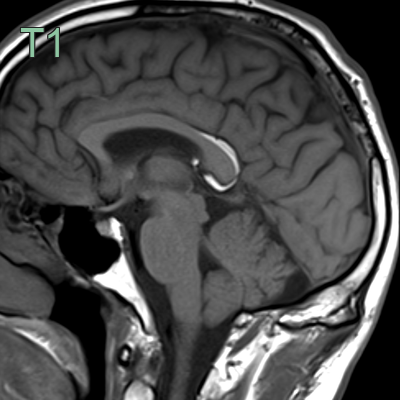
- T1-hyperintense lipoma wrapping around the splenium of the corpus callosum was incidentally indentified.
Treatment¶
- None required for a characteristic asymptomatic lesion, and imaging surveillance is unnecessary
- Surgery is generally avoided because the lesion encases the pericallosal arteries and adheres to neural tissue; reserved for exceptional complications
Differential diagnosis¶
| Differential diagnosis | Differentiating feature |
|---|---|
| Dermoid cyst | More heterogeneous, often off-midline; may rupture and scatter fat droplets through the subarachnoid space and ventricles |
| Teratoma | Mixed solid, cystic, fatty, and calcified components with enhancement and mass effect |
| Falx ossification with fatty marrow | Bone windows show cortex and central marrow rather than a cisternal fat mass |
| Subacute hematoma | T1 hyperintensity does not suppress on fat-sat/Dixon; blood-product susceptibility and evolution over time |
| Thrombosed pericallosal aneurysm | Continuity with the artery and residual flow or enhancement; no macroscopic fat |
-
Truwit et al. Pathogenesis of intracranial lipoma: an MR study in 42 patients. 1990. AJNR. American journal of neuroradiology - Open in new tab. ↩
-
Tart et al. Curvilinear and tubulonodular varieties of lipoma of the corpus callosum: an MR and CT study. 1991. Journal of computer assisted tomography - Open in new tab. ↩