Motor Neurone Disease (MND)¶
Summary
- Progressive neurodegenerative disorder affecting upper and lower motor neurons
- Characterised by muscle weakness, atrophy, and eventual paralysis
- Diagnosis based on clinical presentation, electromyography, and exclusion of other conditions1
Pathophysiology¶
- Degeneration of motor neurons in the brain, brainstem, and spinal cord
- Exact cause unknown, but involves:
- Oxidative stress
- Mitochondrial dysfunction
- Protein aggregation (e.g., TDP-43)
- Glutamate excitotoxicity
- Genetic factors implicated in some cases (e.g., C9orf72, SOD1 mutations)
Demographics¶
- Incidence: 1-2 per 100,000 person-years
- Prevalence: 4-6 per 100,000 population
- Mean age of onset: 55-65 years
- Male to female ratio: 1.5:1
- 5-10% of cases are familial
Diagnosis¶
- Clinical features:
- Progressive muscle weakness and atrophy
- Fasciculations
- Spasticity
- Dysarthria and dysphagia
- Respiratory insufficiency
- Diagnostic criteria:
- El Escorial criteria
- Awaji criteria (includes electrophysiological findings)
- Investigations:
- Electromyography (EMG) and nerve conduction studies
- Blood tests to exclude mimics
- Genetic testing in familial cases
Imaging¶
- Conventional MRI:
- Often normal in early stages
- May show cortical atrophy and hyperintensity of corticospinal tracts on T2-weighted images
- Advanced MRI techniques:
- Diffusion tensor imaging (DTI): Reduced fractional anisotropy in corticospinal tracts
- Functional MRI: Altered activation patterns in motor and extra-motor regions
- Magnetic resonance spectroscopy: Reduced N-acetylaspartate (NAA) in motor cortex
- PET imaging:
- FDG-PET: Hypometabolism in frontal and temporal regions
- PET with radioligands for neuroinflammation (e.g., [11C]-PK11195)
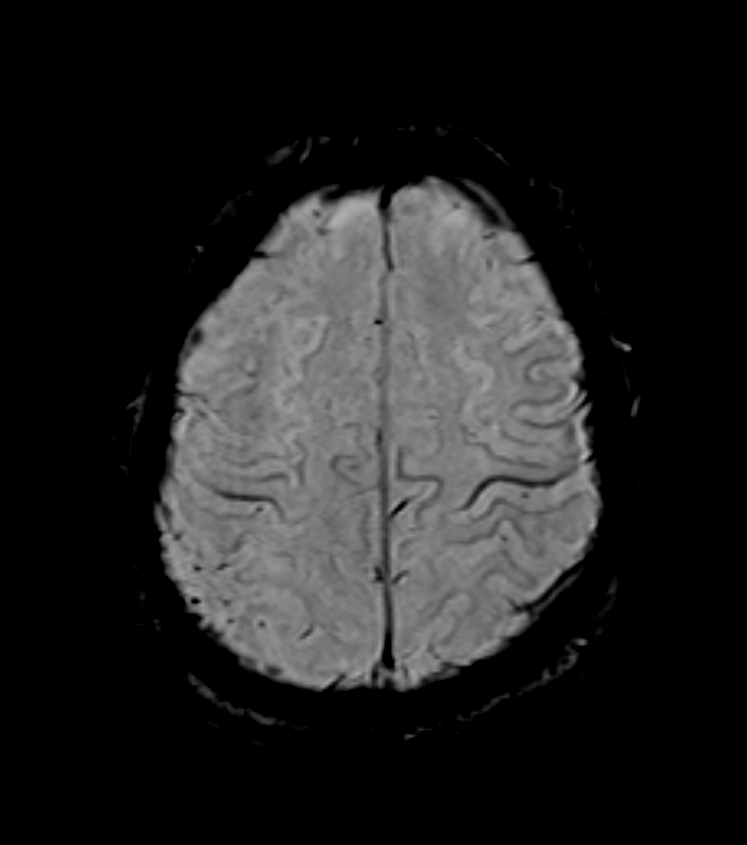
- 70-year-old patient presented with left-sided weakness and spasticity, and executive dysfunction.
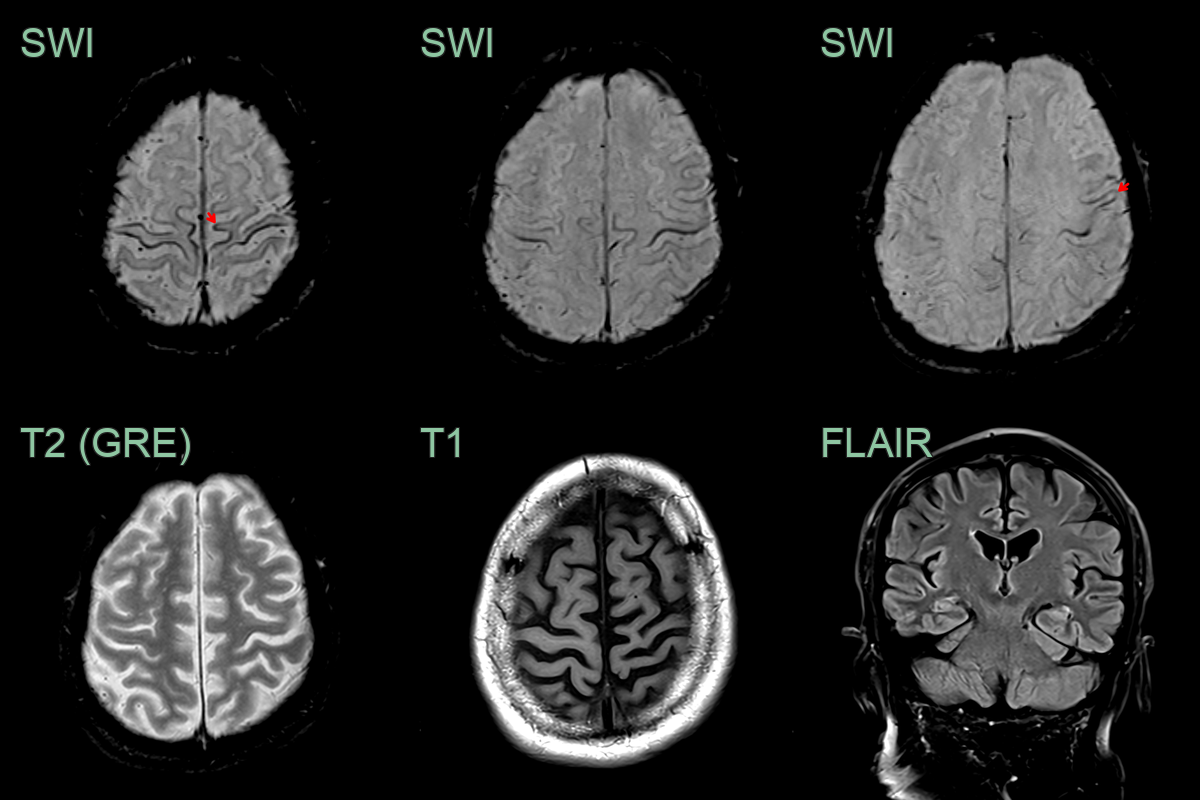
- Excessive susceptibility artefact in the motor cortex (motor band sign) was most apparent around the right hand motor knob.
- There was no significant volume loss or corticospinal tract hyperintensity.
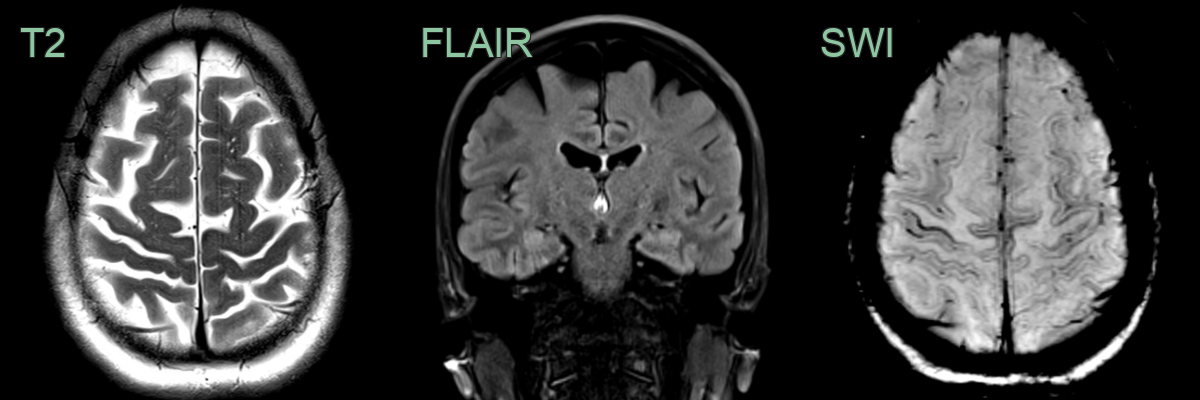
- A 45-year-old patient had a rapidly progressive tetraparesis over 6 months with upper motor signs and tongue fasciculations.
- MRI showed subtle hyperintensity within the corticospinal tracts and excessive susceptibility artefact in the motor cortex.
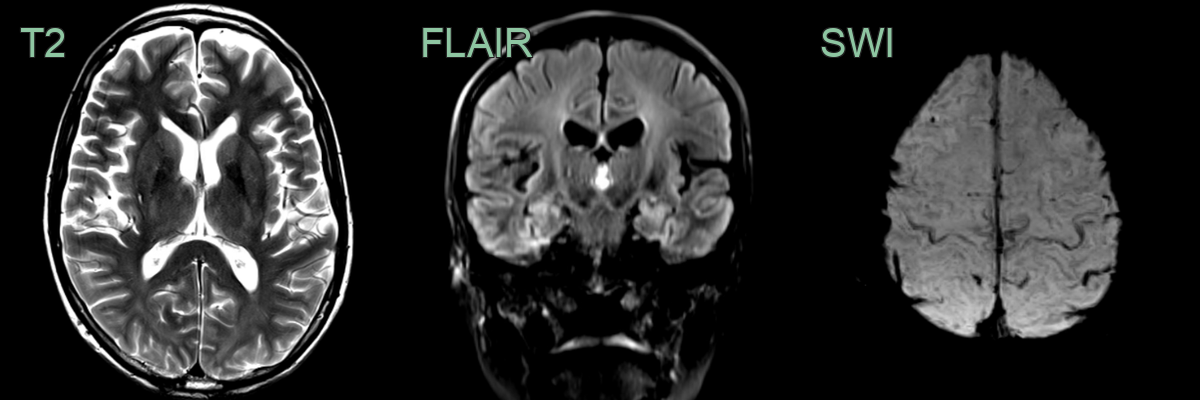
- 65-year-old patient presented with twitching arms and legs, muscle weakness and frequent falls.
- MRI showed marked hyperintensity within the corticospinal tracts and excessive susceptibility artefact in the motor cortex, representing the motor band sign.
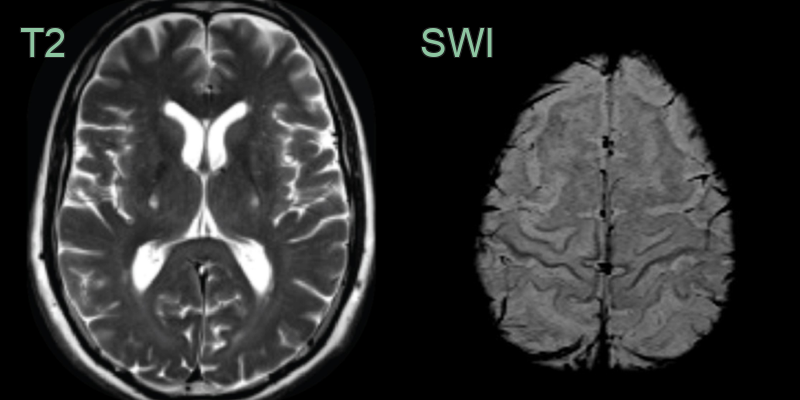
- 60-year-old patient presenting with brisk reflexes, lower limb weakness and tongue fasciculations.
- MRI showed mild parietal volume loss near the vertex and marked susceptibility along the motor cortex that extended anteriorly into the paracentral lobule.
Treatment¶
- Riluzole modestly prolongs survival; care is largely supportive and multidisciplinary
- Imaging clues are the "motor band sign" (motor cortex SWI hypointensity) and corticospinal tract T2 hyperintensity
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Wallerian degeneration | Corticospinal tract T2 hyperintensity in the context of a prior stroke or injury; follows expected degeneration pathway |
| Primary lateral sclerosis | Similar bilateral corticospinal tract T2 hyperintensity and motor band sign; no lower motor neuron involvement |
| Cervical myelopathy | Structural cord compression with degenerative changes on MRI; T2 hyperintensity at the level of compression |
| Multiple sclerosis | Periventricular and juxtacortical demyelinating plaques; Dawson fingers; short spinal cord lesions |
| Hepatic encephalopathy | T1 hyperintensity in globus pallidus; corticospinal tract changes; no motor band sign |
-
Dharmadasa et al. Motor neurone disease. 2018. Handbook of clinical neurology - Open in new tab. ↩