Parotid Abscess¶
Summary
- Parotid abscess is a localised collection of pus within the parotid gland
- Typically results from bacterial infection, often ascending from the oral cavity
- Presents with painful swelling of the parotid region, fever, and trismus1
Pathophysiology¶
- Caused by bacterial infection, most commonly:
- Staphylococcus aureus
- Streptococcus species
- Anaerobic bacteria
- Infection usually ascends from the oral cavity via Stensen's duct
- Risk factors include:
- Dehydration
- Poor oral hygiene
- Immunosuppression
- Ductal obstruction (e.g., sialolithiasis)
- Progression of acute suppurative parotitis if left untreated
Demographics¶
- Can occur at any age, but more common in:
- Elderly patients
- Immunocompromised individuals
- Patients with poor oral hygiene
- No significant gender predilection
- Incidence has decreased with improved dental care and antibiotic use
Diagnosis¶
- Clinical presentation:
- Acute onset of painful swelling in the parotid region
- Fever and malaise
- Trismus (difficulty opening mouth)
- Purulent discharge from Stensen's duct
- Laboratory findings:
- Elevated white blood cell count
- Increased C-reactive protein and erythrocyte sedimentation rate
- Microbiological culture of pus or saliva to identify causative organism
Imaging¶
- Ultrasound:
- First-line imaging modality
- Hypoechoic or anechoic area within the parotid gland
- Internal echoes and septations may be present
- Increased vascularity in surrounding tissues
- CT with contrast:
- Low-density fluid collection with rim enhancement
- Surrounding inflammatory changes and oedema
- Useful for assessing extent and potential complications
- MRI:
- Superior soft tissue contrast
- T1-weighted: hypointense lesion
- T2-weighted: hyperintense lesion with hypointense rim
- Diffusion-weighted imaging: restricted diffusion within abscess
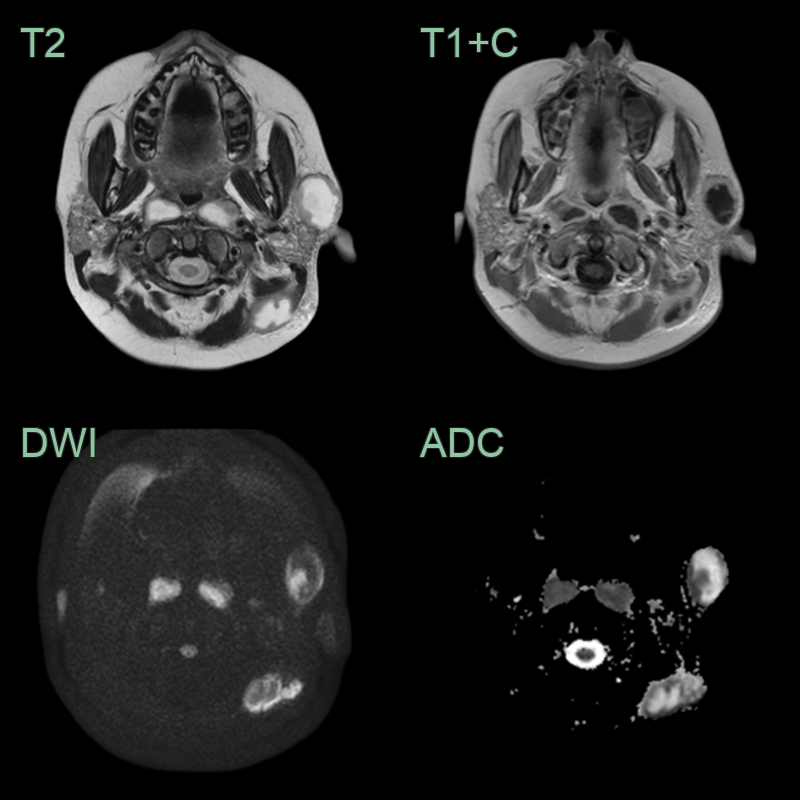
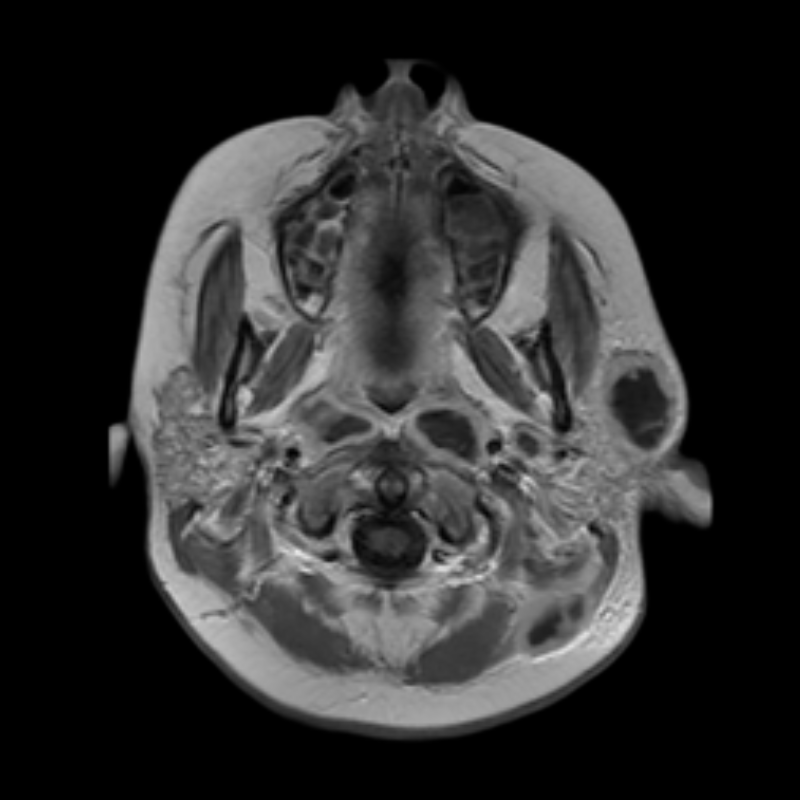
- 35-year-old male presented with a swelling over the left parotid gland.
- MRI showed a peripherally enhancing collection causing diffusion restriction in the left parotid gland.
Treatment¶
- Antibiotics with image-guided aspiration or surgical drainage; a rim-enhancing collection with central restricted diffusion distinguishes abscess from diffuse parotitis
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Acute parotitis (without abscess) | Diffuse gland swelling without discrete fluid collection; no rim enhancement; no restricted diffusion |
| Parotid neoplasm | Solid mass without fluid signal; no rim enhancement; no inflammatory fat stranding |
| Intraparotid lymphadenitis | Discrete lymph nodes within parotid gland; no true glandular abscess cavity |
| Sialolithiasis | Calculus visible in Stensen's duct on CT; may cause duct dilatation without abscess formation |
| Branchial cleft cyst (second) | Well-circumscribed thin-walled cyst at angle of mandible or anterior to SCM; no restricted diffusion; no rim enhancement |
| Masseteric abscess | Collection centred in masseter muscle rather than parotid gland parenchyma |
-
Lakshmi Narayana et al. Parotid abscess in children - A tertiary rural hospital experience. 2015. International journal of pediatric otorhinolaryngology - Open in new tab. ↩