Pembrolizumab Associated Brainstem Encephalitis¶
Summary

- Rare but serious neurological adverse event associated with pembrolizumab immunotherapy
- Characterised by inflammation of the brainstem, leading to various neurological deficits
- Diagnosis based on clinical presentation, MRI findings, and exclusion of other causes1
Pathophysiology¶
- Immune-mediated inflammation of the brainstem triggered by pembrolizumab
- Exact mechanism not fully understood, but likely involves:
- T-cell activation and infiltration of the brainstem
- Cytokine release and local inflammation
- Potential cross-reactivity between tumour antigens and neural tissue
Demographics¶
- Incidence: Rare, estimated at <1% of patients receiving pembrolizumab
- Risk factors:
- Prior history of autoimmune disorders
- Concurrent use of other immunotherapies
- Longer duration of pembrolizumab treatment
Diagnosis¶
- Clinical presentation:
- Acute or subacute onset of neurological symptoms
- Cranial nerve deficits (e.g., diplopia, facial weakness)
- Ataxia and gait disturbances
- Altered mental status
- Laboratory findings:
- CSF analysis: Elevated protein, lymphocytic pleocytosis
- Serum and CSF autoantibody panels (to rule out other causes)
- Exclusion of other etiologies:
- Infectious causes (e.g., viral encephalitis)
- Metastatic disease
- Paraneoplastic syndromes
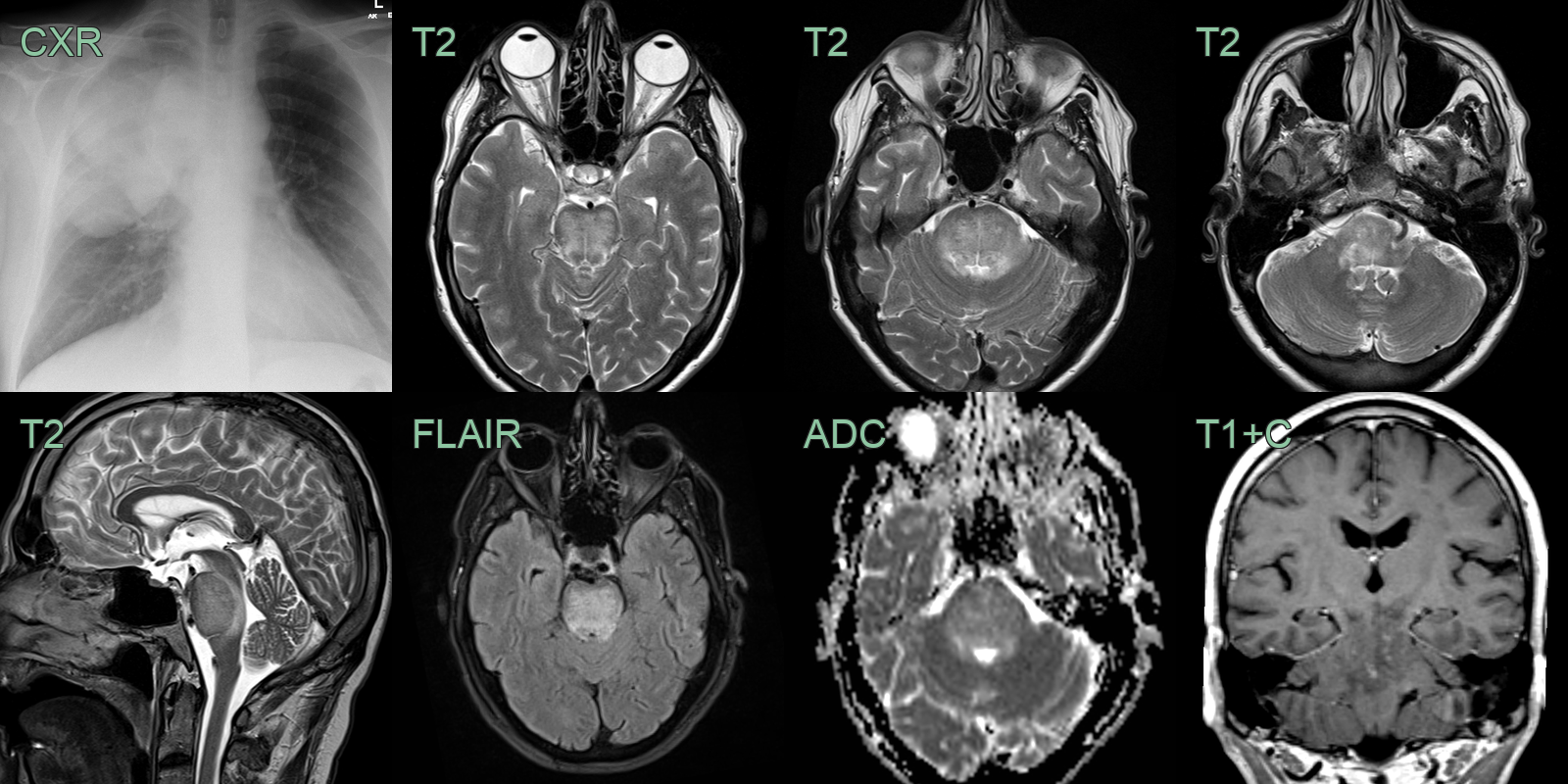
Imaging¶
- MRI brain with contrast:
- T2/FLAIR hyperintensities in the brainstem
- Potential enhancement on T1 post-contrast images
- Diffusion restriction may be present in acute stages
- PET-CT:
- May show hypermetabolism in affected areas of the brainstem
- Differential diagnosis on imaging:
- Brainstem glioma
- Demyelinating disorders (e.g., multiple sclerosis)
- Vascular lesions (e.g., infarction, vasculitis)
Treatment¶
- Stop the checkpoint inhibitor and give high-dose corticosteroids (± IVIG/plasma exchange). Recognising it as an immune-related adverse event, rather than metastatic or infectious disease, is the key
Differential diagnosis¶
| Differential Diagnosis | Distinguishing Feature |
|---|---|
| Brainstem glioma | Expansile infiltrative T2 signal in pons or medulla with mass effect; no associated cerebral hemisphere lesions |
| Brainstem infarction | DWI restriction conforming to vascular territory (basilar perforator, PICA, AICA); associated vessel occlusion on MRA |
| Multiple sclerosis | Focal ovoid demyelinating plaques without mass effect; periventricular and juxtacortical lesions elsewhere |
| Wernicke's encephalopathy | Symmetric T2 hyperintensity in mammillary bodies, periaqueductal grey, and medial thalami |
| CLIPPERS | Punctate and curvilinear perivascular enhancement ("pepper-like") centred on pons and cerebellum |
| Leptomeningeal or parenchymal metastases | Nodular or ring-enhancing lesions with mass effect; other metastatic lesions elsewhere |
-
Buckley et al. Immune-related encephalitis after immune checkpoint inhibitor therapy. 2025. The oncologist - Open in new tab. ↩