Pituitary Microadenoma¶
Summary
- Small (<10 mm) benign tumour arising from the anterior pituitary gland
- May be functional (hormone-secreting) or non-functional
- Often incidentally discovered on imaging; can cause endocrine dysfunction or mass effect1
Pathophysiology¶
- Monoclonal neoplasm arising from adenohypophyseal cells
- Classified based on hormone secretion:
- Prolactinomas (most common)
- Growth hormone-secreting
- ACTH-secreting (Cushing's disease)
- TSH-secreting
- Gonadotropin-secreting
- Non-functioning
- Exact etiology unknown; genetic factors and hormonal stimulation may play a role
Demographics¶
- Prevalence: 10-20% in general population (based on autopsy studies)
- More common in women
- Peak incidence: 30-50 years of age
- Functional adenomas more common in younger patients
Diagnosis¶
- Clinical presentation:
- Asymptomatic (incidental finding)
- Endocrine dysfunction (depending on hormone secretion)
- Headache, visual disturbances (rare in microadenomas)
- Laboratory tests:
- Hormone levels (prolactin, IGF-1, ACTH, cortisol, TSH, free T4)
- Dynamic endocrine testing (e.g., dexamethasone suppression test)
Imaging¶
- MRI:
- Modality of choice for diagnosis and follow-up
- T1-weighted sequences:
- Hypointense compared to normal pituitary tissue
- Best visualised on post-contrast images
- T2-weighted sequences:
- Variable signal intensity
- Dynamic contrast-enhanced imaging:
- Delayed enhancement compared to normal pituitary tissue
- CT:
- Less sensitive than MRI
- May show focal hypodense lesion
- Useful for detecting calcifications or bony changes
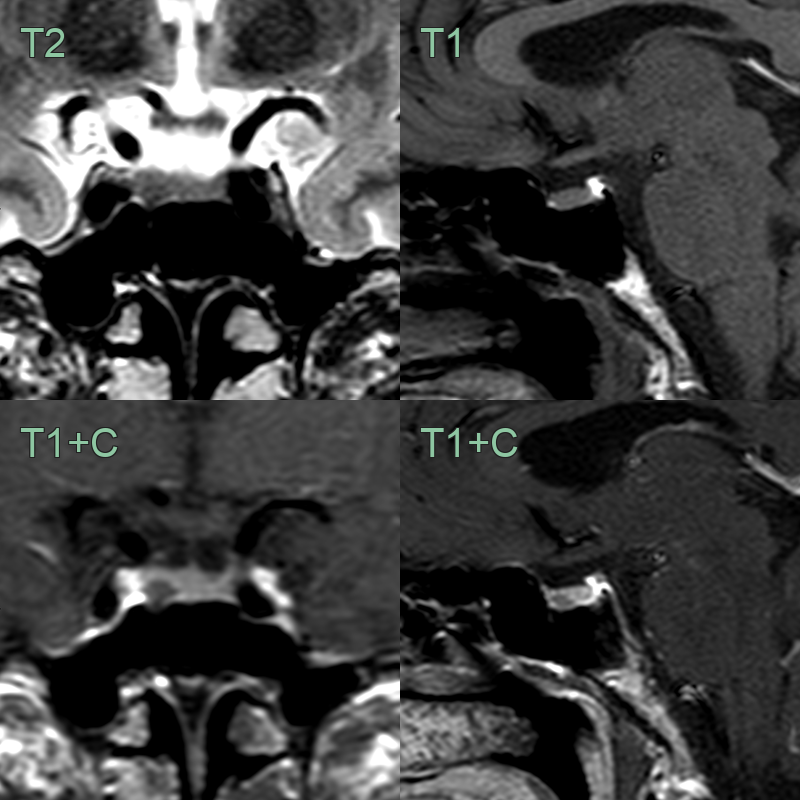
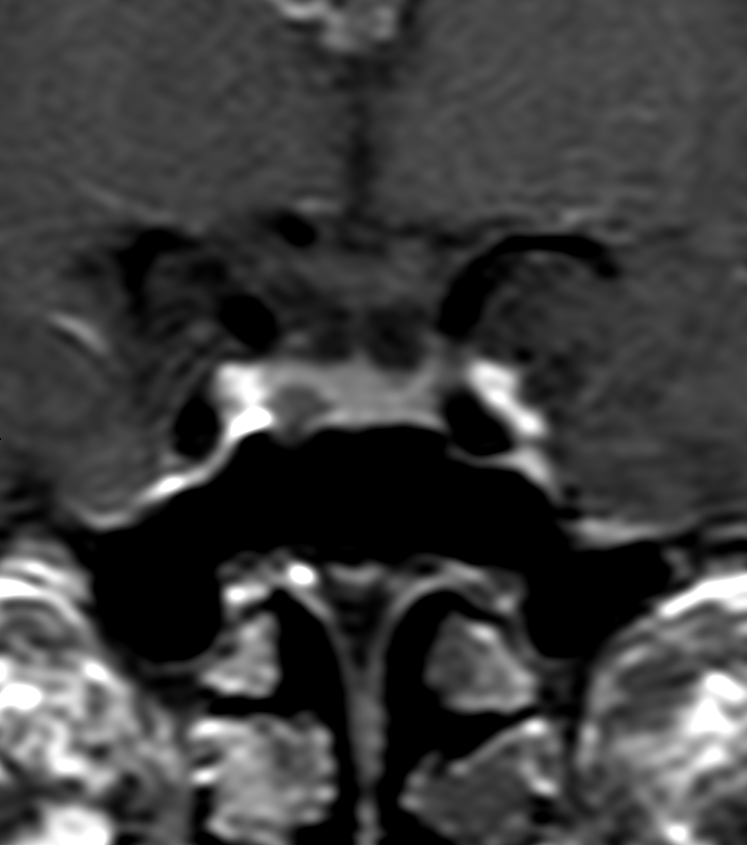
- 50-year-old patient with headaches, joint pain and carpal tunnel syndrome was found to have elevated serum growth factor.
- MRI showed a 4 mm hypoenhancing lesion in the right side of the gland.
- The lesion was only subtly apparent on T2-weighted imaging.
Treatment¶
- Depends on hormone status: dopamine agonists for prolactinomas, transsphenoidal surgery for Cushing's/acromegaly; non-functioning lesions are observed
- Dynamic contrast MRI shows the microadenoma as a focus of delayed enhancement relative to the avidly enhancing normal gland
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Rathke's cleft cyst | Typically midline; no enhancement (rather than hypo-enhancement); T1 and T2 hyperintense signal; intracystic nodule |
-
Melmed et al. Clinical Biology of the Pituitary Adenoma. 2022. Endocrine reviews - Open in new tab. ↩