Radiation Necrosis¶
Summary
- Late complication of radiation therapy characterised by necrosis and oedema of brain tissue
- Typically occurs 6 months to years after treatment
- Imaging findings can mimic tumour recurrence, posing diagnostic challenges1
Pathophysiology¶
- Radiation-induced vascular damage leading to:
- Endothelial cell injury
- Increased vascular permeability
- Ischaemia and hypoxia
- Subsequent tissue necrosis and oedema
- Cytokine-mediated inflammatory response
- White matter demyelination and axonal loss
Demographics¶
- Incidence varies based on radiation dose and technique:
- 3-24% after stereotactic radiosurgery
- 5-15% after conventional fractionated radiotherapy
- Risk factors:
- Higher radiation dose
- Larger treatment volume
- Concurrent chemotherapy
- Younger age at treatment
Diagnosis¶
- Clinical presentation:
- Focal neurological deficits
- Cognitive decline
- Seizures
- Headaches
- Differential diagnosis:
- Tumour recurrence
- Pseudoprogression
- Infection
- Diagnostic challenges:
- Clinical and imaging overlap with tumour recurrence
- Need for multimodal approach
Imaging¶
- MRI:
- T1-weighted: Variable enhancement patterns
- T2/FLAIR: Oedema and mass effect
- DWI: Variable diffusion restriction
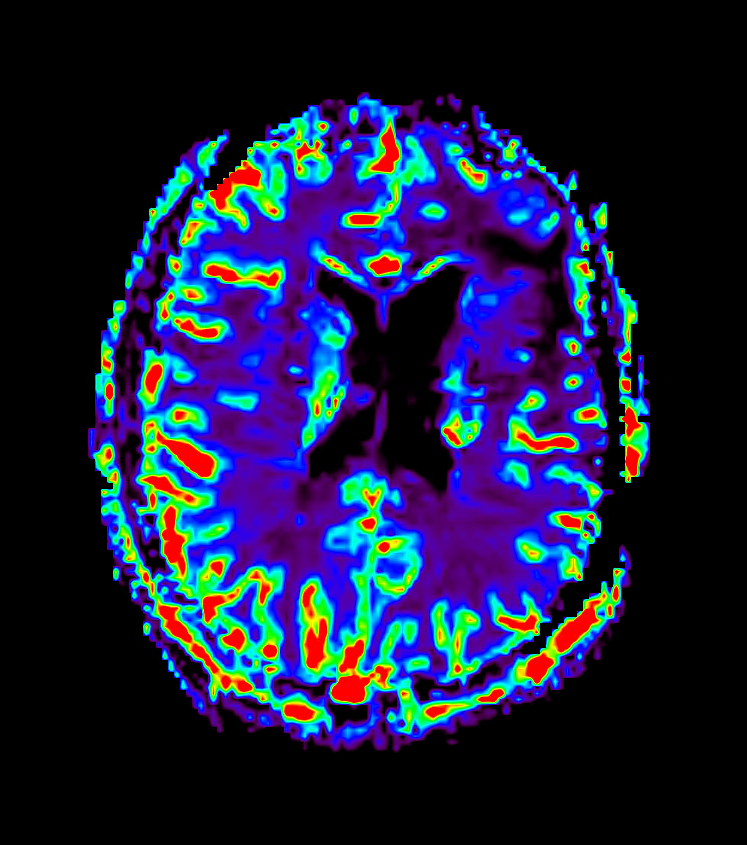
- Perfusion: Typically decreased relative cerebral blood volume (rCBV)
- Advanced imaging techniques:
- MR spectroscopy: Decreased Cho/Cr and NAA/Cr ratios
- PET: Reduced FDG uptake or increased amino acid tracer uptake
- Characteristic features:
- 'Swiss cheese' or 'soap bubble' enhancement pattern
- Lesion crossing white matter tracts
- Corpus callosum involvement
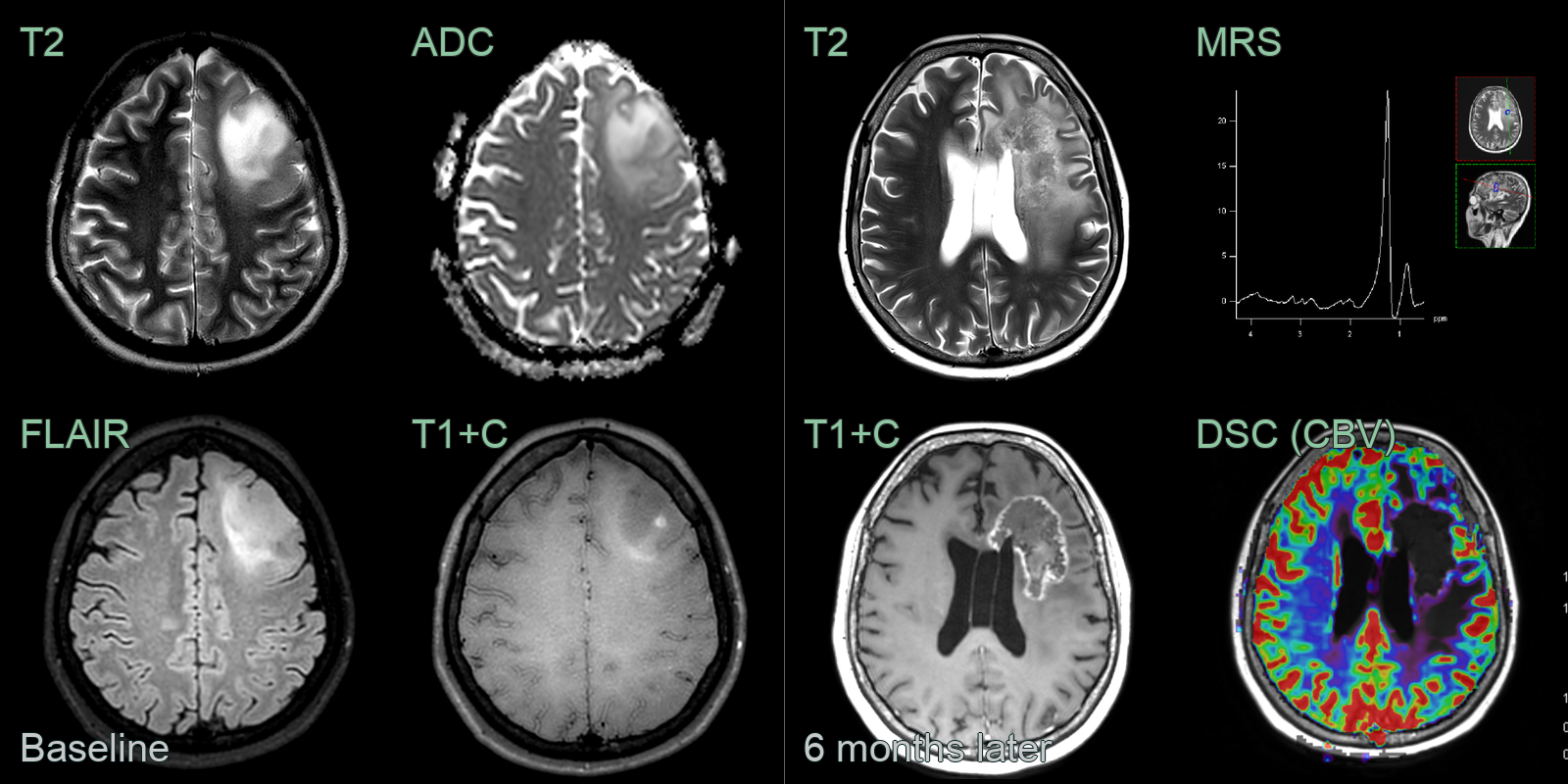
- A 35-year-old patient presented following a seizure.
- MRI showed an ill-defined left frontal lobe lesion with mild diffusion restriction and nodular enhancement.
- Following a resection, a grade 3 astrocytoma was diagnosed.
- The patient had 30 fractions of external beam image guided radiotherapy.
- 6 months later, a heterogeneous and peripherally enhancing lesion developed around the resection cavity. The presence of only a lipid and lactate peaks with little NAA or choline on MR spectroscopy and the low CBV were consistent with treatment related changes, rather than disease progression.
- The peripherally enhancing lesion was unchanged on further follow-up imaging at 1 year.
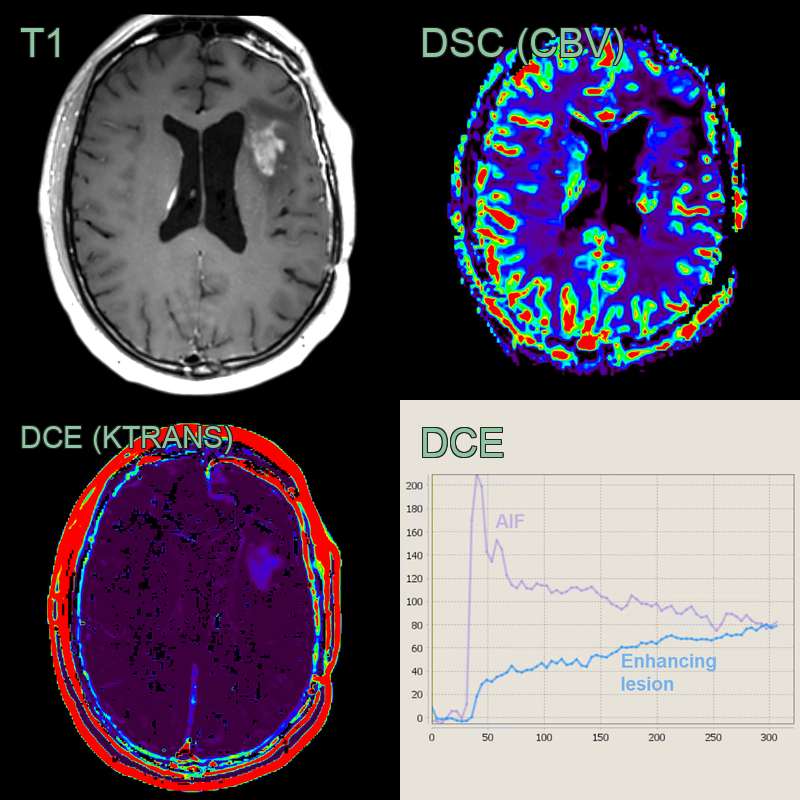
- A 30-year-old patient presented with headache and lethargy.
- A diffuse non-enhancing lesion centred on the left insula that was ultimately diagnosed as a Grade 2 astrocytoma that was treated with debulking, radiation and chemotherapy.
- On 1 year follow-up, the patient was clinically well after surgery but an area of enhancement developed in the left frontal white matter.
- DSC perfusion showed no significant increase in CBV (ratio of ~1.2 relative to contralateral white matter) and a DCE Type 1 curve within the lesion, both of which were compatible with predominantly treatment related effects.
- As expected with treatment related effects, the enhancement regressed over the following year.
Treatment¶
- Corticosteroids and bevacizumab for symptomatic oedema; surgery for refractory or diagnostically uncertain lesions
- Perfusion (low rCBV) and spectroscopy (lipid/lactate rather than choline) help distinguish it from tumour recurrence
Differential diagnosis¶
| Imaging differential | Differentiating feature |
|---|---|
| Tumour recurrence / pseudoprogression | Recurrence shows high rCBV on perfusion; radiation necrosis gives "soap bubble"/"Swiss cheese" enhancement with low rCBV and a lipid/lactate-dominant spectrum |
| Abscess | Thin smooth ring enhancement; restricted central DWI; satellite lesions; no prior radiation |
| Metastasis | Located at grey-white junction; ring or nodular enhancement; multiple lesions; not confined to radiation field |
| Subacute infarct | Follows a vascular territory; wedge-shaped; gyral enhancement; DWI restriction in acute/subacute phase |
| Progressive multifocal leukoencephalopathy | Subcortical U-fibre involvement; restricted DWI at active edge; no enhancement; no prior radiation |
| Encephalitis | Cortical and limbic T2 signal; temporal lobe predilection; not confined to radiation field |
| Demyelinating disease | Ovoid periventricular lesions; incomplete ring enhancement; not confined to radiation field |
-
Furuse et al. Delayed brain radiation necrosis: pathological review and new molecular targets for treatment. 2015. Medical molecular morphology - Open in new tab. ↩