Spinal Dural Arteriovenous Fistula (DAVF)¶
Summary

- Abnormal arteriovenous shunt between radiculomeningeal artery and radicular vein within dura mater, causing venous congestion and progressive myelopathy
- Presents with progressive lower extremity weakness, sensory changes, and bowel/bladder dysfunction
- MRI shows T2 hyperintense cord signal with perimedullary flow voids and cord enhancement1
Pathophysiology¶
- Acquired lesion with direct arteriovenous shunt typically at nerve root sleeve level
- Arterial feeder (usually single radiculomeningeal artery) connects directly to radicular vein
- Arterialized venous flow causes venous hypertension in coronal venous plexus
- Venous congestion leads to:
- Decreased arteriovenous pressure gradient
- Reduced tissue perfusion
- Chronic hypoxia and oedema
- Progressive myelopathy (Foix-Alajouanine syndrome)
- Most commonly located in thoracolumbar region (T6-L2)
Demographics¶
- Most common spinal vascular malformation (60-80% of all spinal AVMs)
- Male predominance (5:1 ratio)
- Peak incidence: 5th-6th decade
- Rare in patients under 30 years
- Risk factors:
- Previous spinal trauma
- Prior surgery
- Unknown in most cases (idiopathic)
Diagnosis¶
- Clinical presentation:
- Insidious onset with progressive symptoms
- Ascending myelopathy
- Lower extremity weakness (symmetric or asymmetric)
- Sensory disturbances (paresthesias, numbness)
- Bowel and bladder dysfunction
- Erectile dysfunction in males
- Symptoms may worsen with exercise (venous congestion)
- Physical examination:
- Upper motor neuron signs below lesion level
- Hyperreflexia
- Positive Babinski sign
- Sensory level may be present
Imaging¶
-
MRI Spine:
- T2: Hyperintense intramedullary signal (cord oedema), typically involving multiple segments with predominant central/centromedullary distribution
- T2: Perimedullary flow voids (dilated veins) appearing as serpentine hypointense structures on dorsal cord surface
- T1: Normal or slightly hypointense cord signal
- T1+C: Patchy intramedullary enhancement (subacute cases), enhancement of perimedullary vessels
- DWI: Usually normal (helps differentiate from acute infarction)
- MRA: May demonstrate enlarged perimedullary vessels and early draining vein
-
CT Angiography:
- Dilated perimedullary veins
- May identify feeding artery level
- Less sensitive than MRI for cord changes
-
Digital Subtraction Angiography (DSA):
- Gold standard for diagnosis and treatment planning
- Identifies:
- Feeding radiculomeningeal artery
- Fistula location
- Draining radicular vein
- Dilated coronal venous plexus
- Prolonged venous phase
- Absence of nidus (differentiates from AVM)
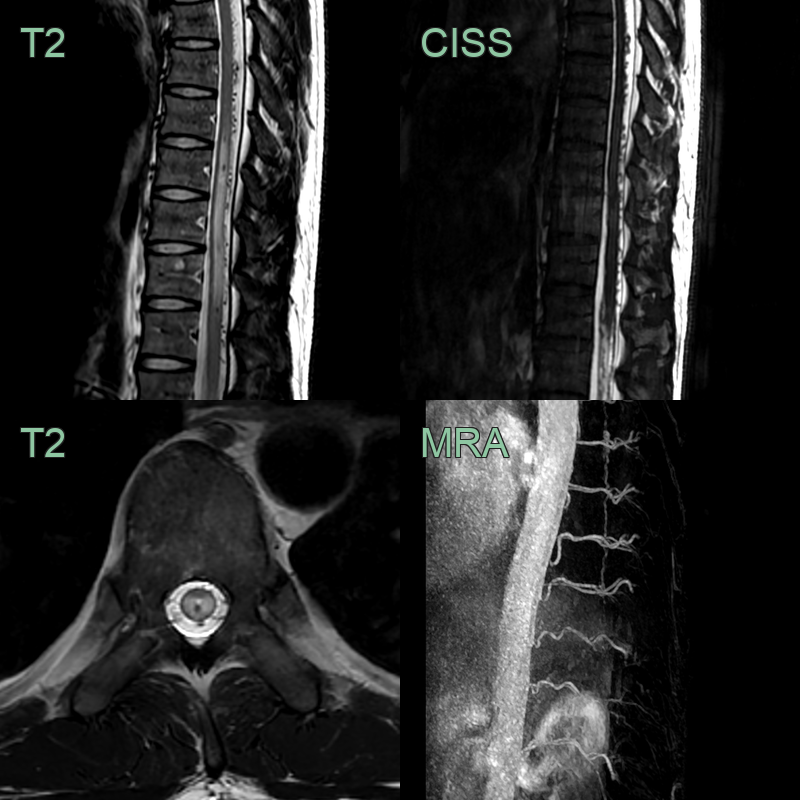
- A 50-year-old male presented with a 6 month history of progressively worsening spasticity and weakness in both legs.
- MRI showed distal cord hyperintensity and many extramedullary flow voids.
- Time-resolved MRA showed early arterial filling of a vessel running along the ventral cord.
Treatment¶
- Endovascular embolisation or surgical disconnection of the fistula; early treatment prevents irreversible myelopathy
- The combination of central cord T2 oedema with dorsal perimedullary flow voids is the key imaging clue to this frequently missed, treatable cause of myelopathy
Differential diagnosis¶
| Differential diagnosis | Differentiating feature |
|---|---|
| Spinal cord tumour | Intramedullary expansile mass with cord enlargement and heterogeneous enhancement; no perimedullary flow voids |
| Transverse myelitis | Absence of perimedullary flow voids on MRI; cord swelling and enhancement; no serpiginous vascular structures |
| Multiple sclerosis | Multiple periventricular and juxtacortical white matter lesions on brain MRI; short cord lesions without perimedullary flow voids |
| Spinal cord infarction | Restricted diffusion on DWI with owl-eye or pencil-like pattern; absence of perimedullary flow voids; anterior cord predilection |
| Subacute combined degeneration (B12 deficiency) | Dorsal column predominant signal change with inverted V sign on axial MRI; no perimedullary flow voids |
| Spinal arteriovenous malformation (AVM) | Intramedullary nidus visible on angiography; multiple feeders rather than a single fistulous connection |
| Chronic inflammatory demyelinating polyneuropathy (CIDP) | Nerve root enhancement on post-contrast MRI rather than cord signal change; no perimedullary flow voids |
| Radiation myelopathy | T2 signal change and cord atrophy confined to the radiation treatment field; no perimedullary flow voids |
-
C Koch. Spinal dural arteriovenous fistula. 2006. Current opinion in neurology - Open in new tab. ↩