Spinal Meningioma¶
Summary
- Slow-growing, benign tumours arising from arachnoid cap cells of the spinal meninges
- Most common intradural extramedullary spinal tumour in adults
- Typically presents with gradual onset of neurological symptoms due to spinal cord compression1
Pathophysiology¶
- Arise from arachnoid cap cells in the spinal meninges
- Most commonly occur in the thoracic spine (80%), followed by cervical and lumbar regions
- Grow slowly, causing gradual compression of the spinal cord and nerve roots
- WHO classification:
- Grade I (benign): 90% of cases
- Grade II (atypical): 5-7% of cases
- Grade III (anaplastic): <1% of cases
Demographics¶
- Peak incidence: 40-70 years of age
- Female predominance (female:male ratio 3-4:1)
- Account for 25-46% of primary spinal cord tumours in adults
- Rare in children, comprising <5% of paediatric spinal tumours
Diagnosis¶
- Clinical presentation:
- Gradual onset of neurological symptoms
- Local or radicular pain
- Sensory disturbances
- Motor weakness
- Gait abnormalities
- Sphincter dysfunction (in advanced cases)
- Physical examination:
- Sensory level deficit
- Motor weakness below the level of the lesion
- Hyperreflexia and spasticity
- Positive Babinski sign
Imaging¶
- MRI: imaging modality of choice
- T1-weighted: iso- to hypointense relative to spinal cord
- T2-weighted: iso- to hyperintense
- Strong, homogeneous enhancement with gadolinium
- "Dural tail" sign often present
- May demonstrate calcifications (10-20% of cases)
- CT:
- Useful for detecting calcifications and bony changes
- May show scalloping of adjacent vertebral bodies in long-standing cases
- Plain radiographs:
- Limited utility, may show bony erosion or widening of neural foramina

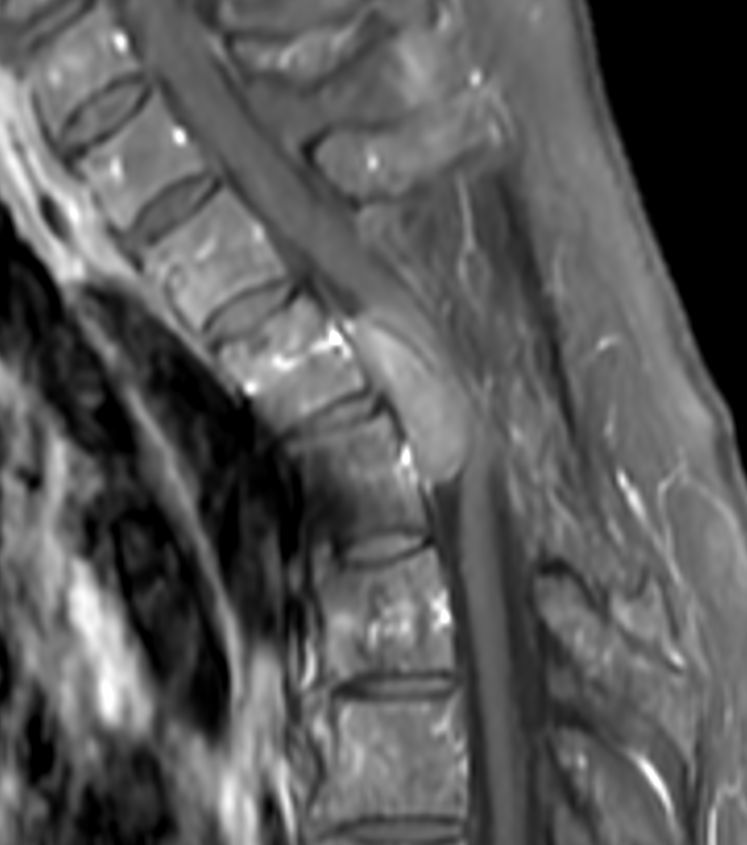
- A 60-year-old patient presented with low limb sensory disturbance.
- MRI showed a hypointense lesion with a broad thecal base compressing the thoracic cord.
Treatment¶
- Surgical resection, usually curative. It is the commonest intradural-extramedullary tumour, typically a broad-based, dural-tailed, thoracic enhancing mass in a middle-aged woman
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Schwannoma | Typically eccentric to the spinal cord, often with "dural tail" sign absent |
| Neurofibroma | Dumbbell-shaped expansion through neural foramen; "target sign" on T2; may be multiple |
| Metastatic tumour | Often multiple lesions; may have associated bony involvement; more aggressive bone destruction |
| Ependymoma | Intramedullary location; often with syringomyelia; "cap sign" haemosiderin on SWI |
| Astrocytoma | Intramedullary location; poorly defined margins; irregular enhancement |
| Lymphoma | Homogeneous epidural or intradural mass; restricted diffusion on DWI; may be multiple |
| Spinal epidural abscess | Rim-enhancing collection; restricted diffusion in abscess; cord compression without intradural involvement |
| Herniated disc | Typically at disc level, associated degenerative changes |
| Arachnoid cyst | No enhancement, CSF-like signal on all sequences |
| Spinal arteriovenous malformation | Flow voids on MRI, associated cord oedema |
-
Sadrameli et al. Resection of Spinal Meningioma Using Ultrasonic BoneScalpel Microshaver: Cases, Technique, and Review of the Literature. 2020. Operative neurosurgery (Hagerstown, Md.) - Open in new tab. ↩