Spinal Schwannoma¶
Summary
- Benign nerve sheath tumour arising from Schwann cells of spinal nerve roots
- Typically presents with radicular pain, sensory changes, and/or motor weakness
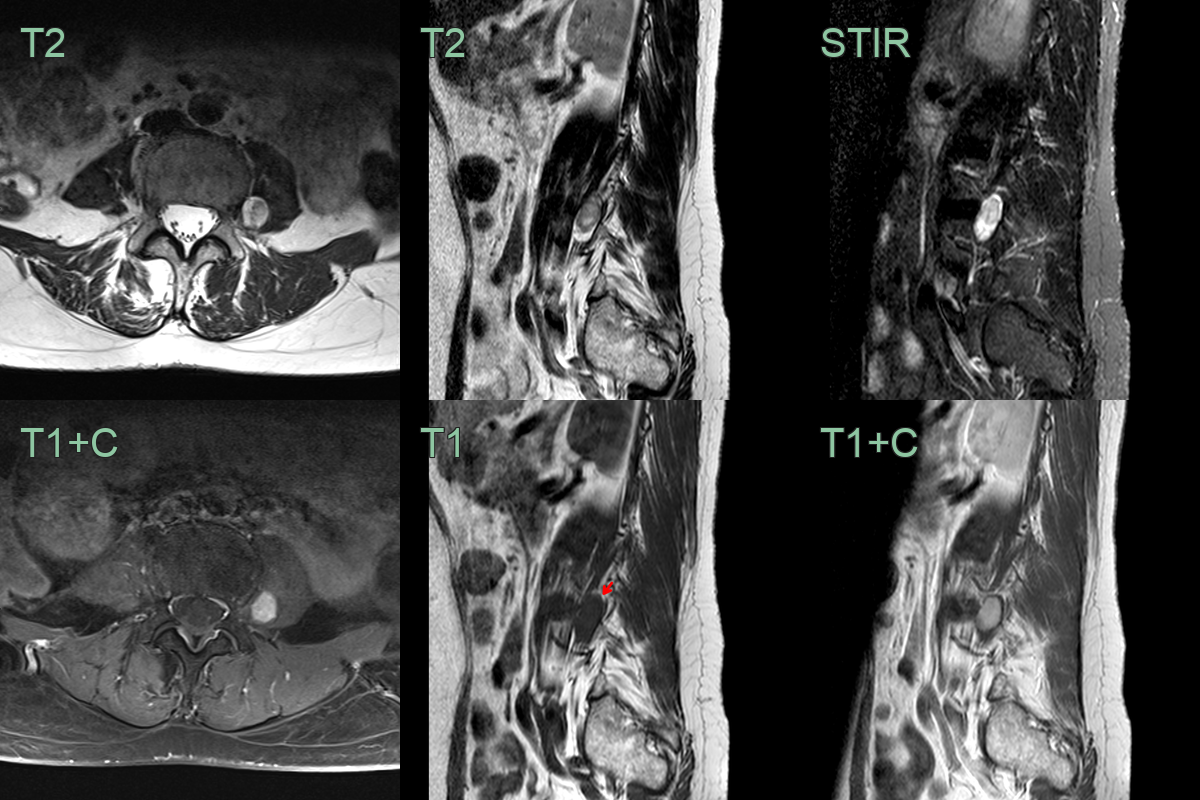
- Characteristic imaging findings include a well-circumscribed, enhancing intradural-extramedullary mass1
Pathophysiology¶
- Originates from Schwann cells of spinal nerve roots
- Usually solitary, but can be multiple in neurofibromatosis type 2 (NF2)
- Slow-growing tumours that compress adjacent neural structures
- Histologically characterised by Antoni A (cellular) and Antoni B (loose) areas
Demographics¶
- Accounts for 30% of primary spinal tumours
- Most common in adults aged 40-60 years
- No significant gender predilection
- Increased incidence in patients with NF2
Diagnosis¶
- Clinical presentation:
- Radicular pain along the affected nerve root
- Sensory changes in the corresponding dermatome
- Motor weakness in severe cases
- Myelopathy if spinal cord compression occurs
- Physical examination:
- Neurological deficits corresponding to the affected spinal level
- Possible signs of myelopathy in advanced cases
Imaging¶
- MRI:
- T1-weighted: isointense to hypointense relative to spinal cord
- T2-weighted: hyperintense
- Contrast-enhanced: strong, homogeneous enhancement
- "Target sign" on axial T2: central hypointensity with peripheral hyperintensity
- CT:
- Isodense to hypodense soft tissue mass
- Possible widening of neural foramen or scalloping of vertebral bodies
- Plain radiographs:
- May show widening of neural foramen or scalloping of vertebral bodies in large tumours
Treatment¶
- Surgical resection is curative. A well-defined, avidly enhancing intradural-extramedullary mass with a "target sign" and neural foraminal ("dumbbell") extension is typical; multiple schwannomas suggest NF2
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Meningioma | Typically dural-based, often calcified, and enhances homogeneously |
| Neurofibroma | "Target sign" on T2-weighted MRI (central low, peripheral high); dumbbell-shaped neural foramen expansion; may be multiple |
| Ependymoma | Intramedullary location; often with associated syrinx; haemosiderin "cap sign" on SWI |
| Metastasis | Multiple lesions; may show associated bony involvement; more aggressive growth pattern |
| Herniated disc | Typically at disc level; follows disc signal on T2; no contrast enhancement |
| Spinal arteriovenous malformation | Flow voids on MRI; associated cord oedema; serpiginous vessels on surface |
| Arachnoid cyst | No contrast enhancement; CSF signal on all sequences including FLAIR |
| Epidural abscess | Rim-enhancing collection; restricted diffusion in cavity; associated cord compression |
| Spinal cord lipoma | Fat signal on all MRI sequences, no contrast enhancement |
| Tarlov cyst | Occurs along nerve roots, typically in sacral region |
-
Hajikarimloo et al. Preoperative Differentiation of Spinal Schwannoma and Meningioma Using Machine Learning-Based Models: A Systematic Review and Meta-Analysis. 2025. World neurosurgery - Open in new tab. ↩