Transient Global Amnesia (TGA)¶
Summary
- Acute, temporary loss of anterograde memory with preserved retrograde memory
- Typically lasts 4-6 hours, resolving within 24 hours
- Characteristic imaging findings on diffusion-weighted MRI1
Pathophysiology¶
- Exact mechanism remains unclear, but leading hypotheses include:
- Transient ischaemia in the medial temporal lobe
- Venous congestion leading to hippocampal dysfunction
- Migraine-related phenomenon
- Hippocampal CA1 region particularly vulnerable to metabolic stress
Demographics¶
- Incidence: 5-10 per 100,000 persons per year
- Peak age: 50-70 years
- Slight female predominance (1.2:1 female-to-male ratio)
- Rare in individuals under 40 years of age
Diagnosis¶
- Clinical diagnosis based on:
- Sudden onset of anterograde amnesia
- Preserved retrograde memory
- No focal neurological deficits
- Resolution within 24 hours
- Exclusion of other causes (e.g., stroke, seizure, head trauma)
- Diagnostic criteria proposed by Hodges and Warlow
Imaging¶
- CT:
- Usually normal
- Useful to exclude other pathologies (e.g., haemorrhage)
- MRI:
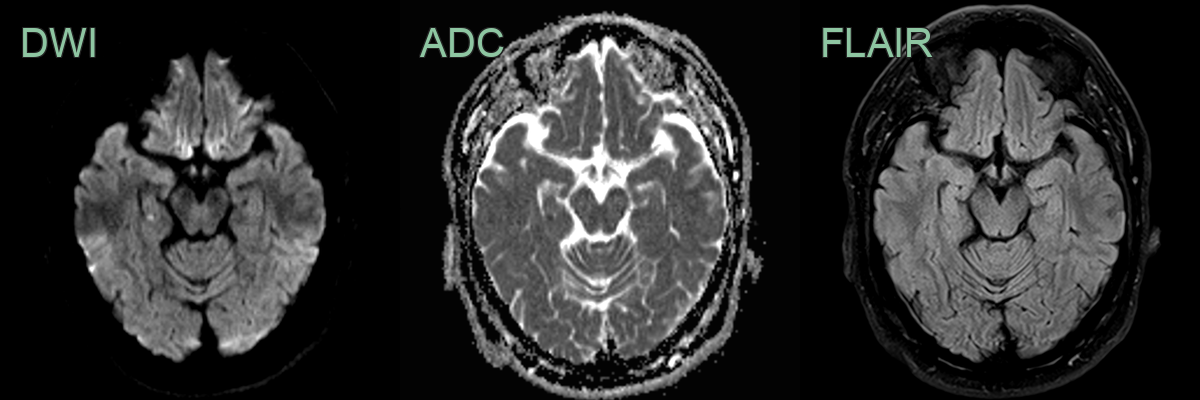
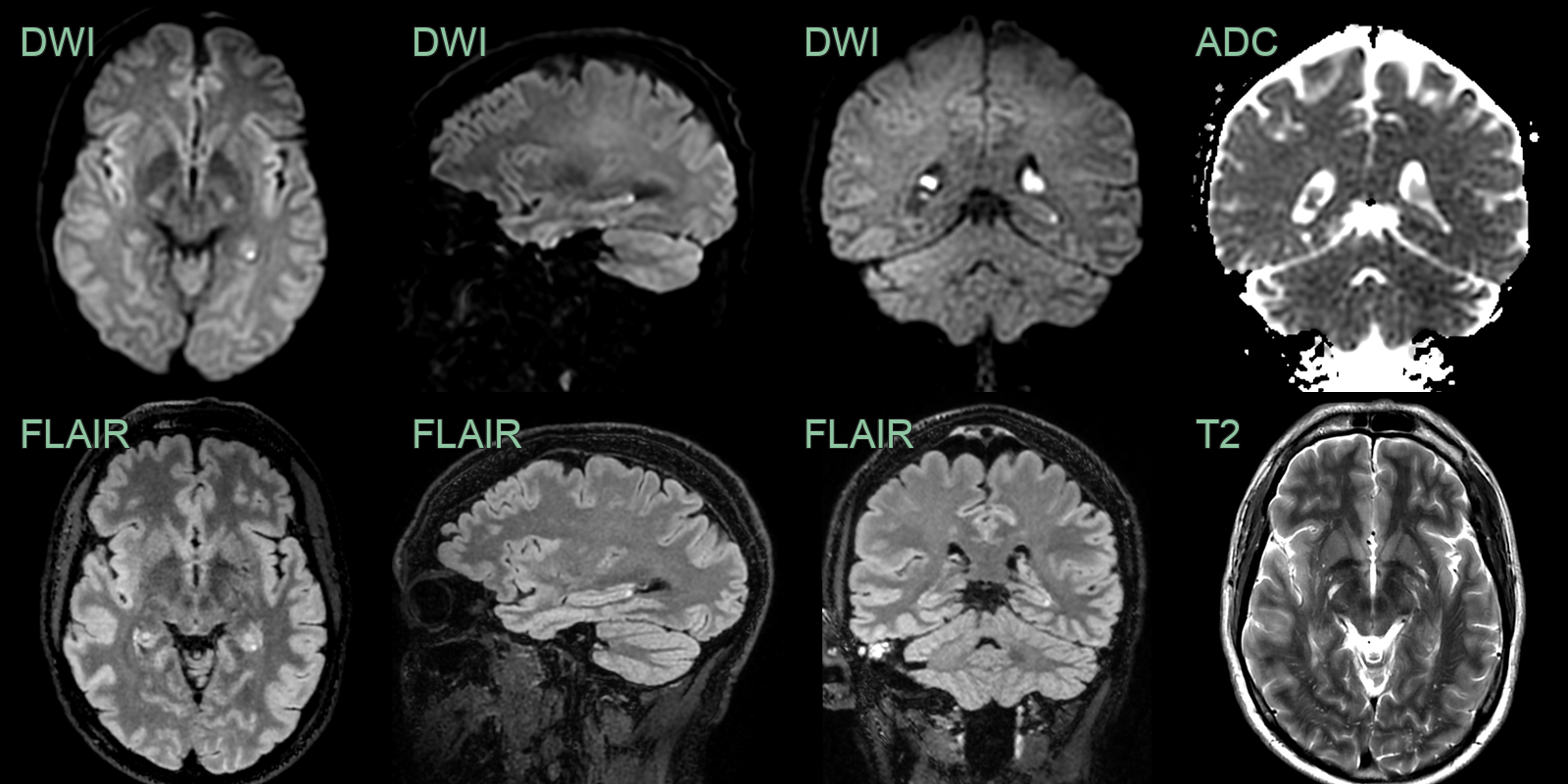
- Diffusion-weighted imaging (DWI):
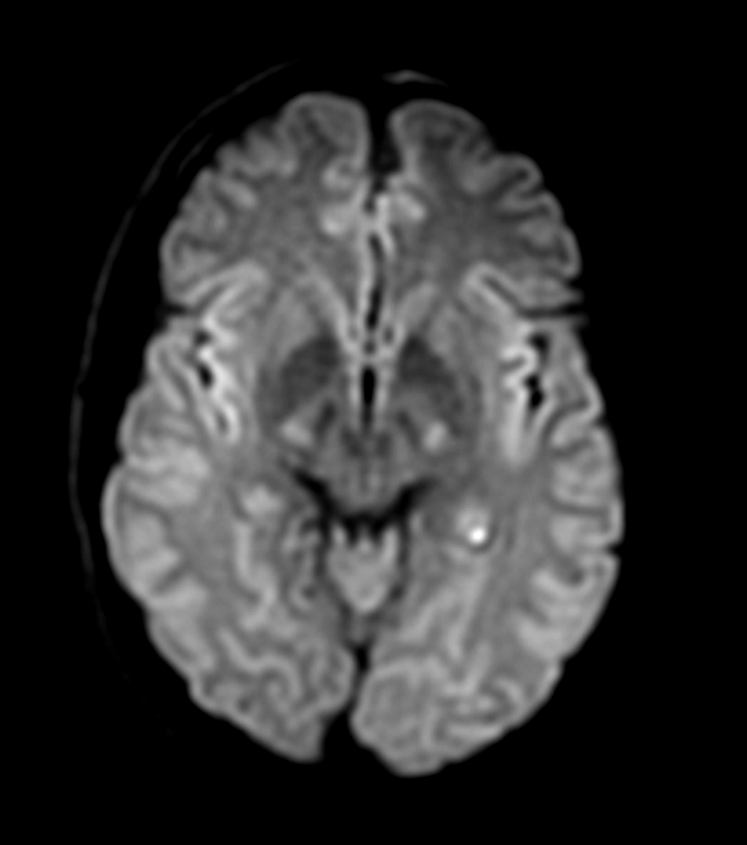
- Characteristic punctate 1-3 mm hyperintense lesions in lateral hippocampus
- Typically unilateral (60-70%) or bilateral (30-40%)
- Best visualised 24-72 hours after symptom onset
- T2-weighted and FLAIR:
- May show corresponding hyperintensities, but less sensitive than DWI
- Functional imaging:
- PET and SPECT may show transient hypoperfusion in medial temporal lobes
- 55-year-old male presenting with 24 hours of anterograde amnesia.
- DWI showed a focus of diffusion restriction in body of the right hippocampus.
- A 50-year-old patient presented with sudden onset confusion and anterograde amnesia followed by a headache (that differed from usual migraine).
- MRI showed a punctate diffusion-weighted hyperintensity, with some degree of restriction, in the tail of the left hippocampus.
Treatment¶
- None required; self-limiting with a good prognosis. The punctate DWI dot in the lateral hippocampus (CA1) is best seen at 24–72 hours and may be absent if imaged too early
Differential diagnosis¶
| Differential Diagnosis | Distinguishing Feature |
|---|---|
| Acute hippocampal infarct | Persisting restricted diffusion in a PCA/anterior choroidal territory; larger or irregular lesion |
| Limbic encephalitis | More generalised medial temporal T2/FLAIR hyperintensity without the focal punctate DWI spot of TGA |
| Herpes simplex encephalitis | Asymmetric medial temporal swelling with haemorrhage and leptomeningeal enhancement |
| Status epilepticus (mesial temporal) | Hippocampal/cortical swelling with FLAIR hyperintensity and restricted diffusion beyond CA1 |
-
A Ropper. Transient Global Amnesia. 2023. The New England journal of medicine - Open in new tab. ↩