Trigeminal Neuralgia¶
Summary
- Chronic neuropathic pain disorder affecting the trigeminal nerve
- Characterised by sudden, severe, electric shock-like pain in the face
- Diagnosis primarily clinical, with MRI to rule out secondary causes1
Pathophysiology¶
- Neurovascular compression of the trigeminal nerve root entry zone, most commonly by superior cerebellar artery
- Demyelination of trigeminal sensory fibres leading to ephaptic transmission
- Central sensitization and hyperexcitability of trigeminal nuclei
Demographics¶
- Incidence: 4-13 per 100,000 person-years
- Peak onset: 50-60 years of age
- Female to male ratio: 1.5-2:1
- Higher prevalence in patients with multiple sclerosis (1-6.3%)
Diagnosis¶
- Based on clinical presentation and patient history
- International Headache Society diagnostic criteria:
- At least three attacks of unilateral facial pain
- Occurring in one or more divisions of the trigeminal nerve
- Pain has at least three of the following characteristics:
- Recurring in paroxysmal attacks
- Severe intensity
- Electric shock-like, shooting, stabbing, or sharp in quality
- Lasting from a fraction of a second to 2 minutes
- Triggered by innocuous stimuli
- No clinically evident neurological deficit
Imaging¶
- MRI brain with contrast:
- To exclude secondary causes (e.g., tumours, multiple sclerosis)
- High-resolution T2-weighted sequences to visualise neurovascular compression
- MR angiography:
- To evaluate vascular anatomy and identify compressing vessels
- DTI and tractography:
- To assess microstructural changes in trigeminal nerve
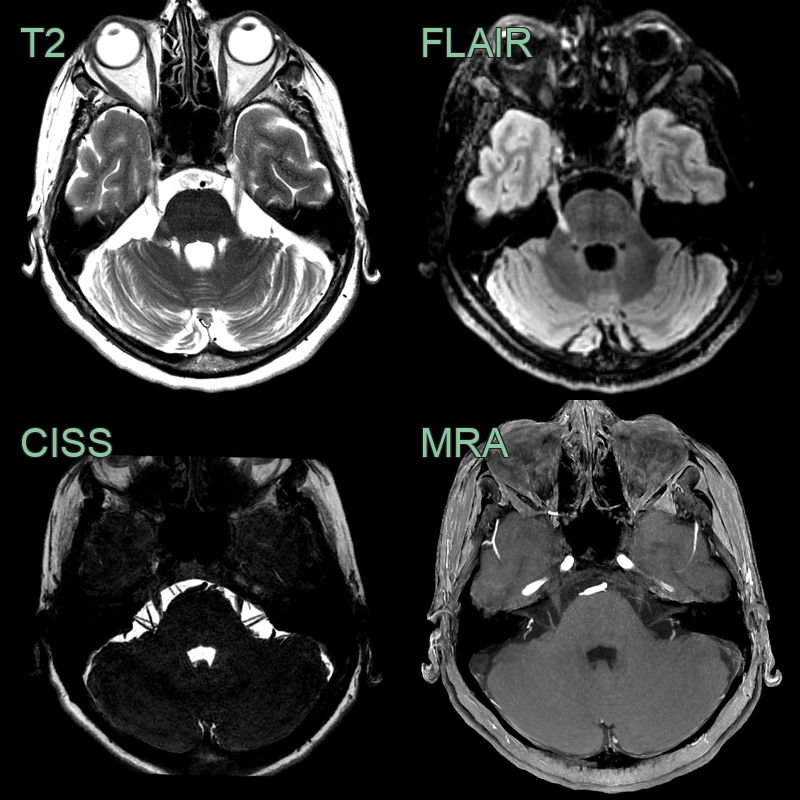
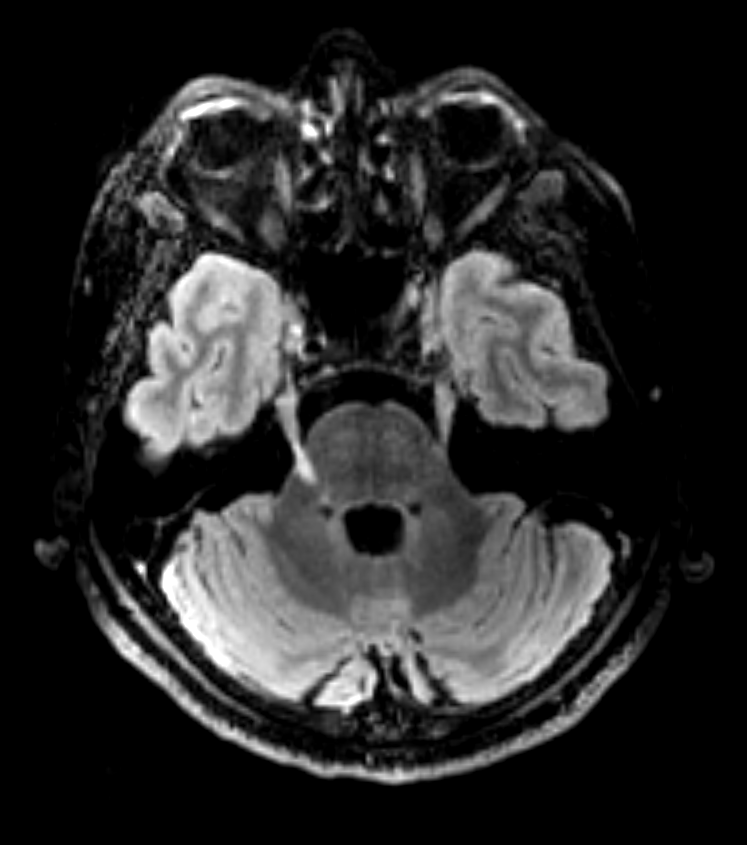
- 50-year-old patient with multiple sclerosis presented with a 6 month history of right sided trigeminal neuralgia.
- A T2-hyperintense demyelinating lesion in the right hemipons corresponds to intraparenchymal fascicles of the trigeminal nerve.
Treatment¶
- Carbamazepine first-line; microvascular decompression for refractory cases with a compressing vessel
- MRI is done to identify neurovascular compression at the root entry zone and to exclude a secondary cause (tumour or MS plaque)
-
Bendtsen et al. Advances in diagnosis, classification, pathophysiology, and management of trigeminal neuralgia. 2020. The Lancet. Neurology - Open in new tab. ↩