Vertebral Haemangioma¶
Summary
- Benign vascular tumour of the spine, composed of thin-walled blood vessels and fatty tissue
- Usually asymptomatic, incidentally found on imaging
- Characteristic "polka-dot" appearance on CT and hyperintense signal on T1-weighted MRI1
Pathophysiology¶
- Hamartomatous lesion of vascular origin
- Composed of:
- Thin-walled blood vessels
- Fatty tissue
- Fibrous stroma
- Slow-growing, with potential for expansion and bone remodeling
- Rarely causes vertebral body expansion or extraosseous extension
Demographics¶
- Prevalence: 10-12% of the general population
- Most common in adults aged 30-50 years
- Slight female predominance
- Can occur in any vertebra, but most common in:
- Thoracic spine (60-70%)
- Lumbar spine (20-30%)
- Cervical spine (rarely affected)
Diagnosis¶
- Often asymptomatic and incidentally discovered on imaging
- Symptomatic cases may present with:
- Local pain
- Radiculopathy
- Myelopathy (in cases of spinal cord compression)
- Physical examination usually unremarkable
- Differential diagnosis includes:
- Metastatic disease
- Multiple myeloma
- Lymphoma
- Eosinophilic granuloma
Imaging¶
X-ray¶
- Coarse vertical trabeculation ("corduroy" appearance)
- Thickened trabeculae may create a "honeycomb" pattern
CT¶
- Characteristic "polka-dot" appearance on axial images
- Represents thickened trabeculae surrounded by low-density fatty tissue
- Coarse vertical trabeculation on sagittal and coronal reconstructions
MRI¶
- T1-weighted: Hyperintense signal due to fat content
- T2-weighted: Hyperintense signal
- STIR: Variable signal suppression depending on fat content
- Contrast enhancement: Usually present, may be intense and homogeneous
Nuclear Medicine¶
- Bone scintigraphy: Usually photopenic ("cold") lesion
- FDG-PET: Typically low uptake
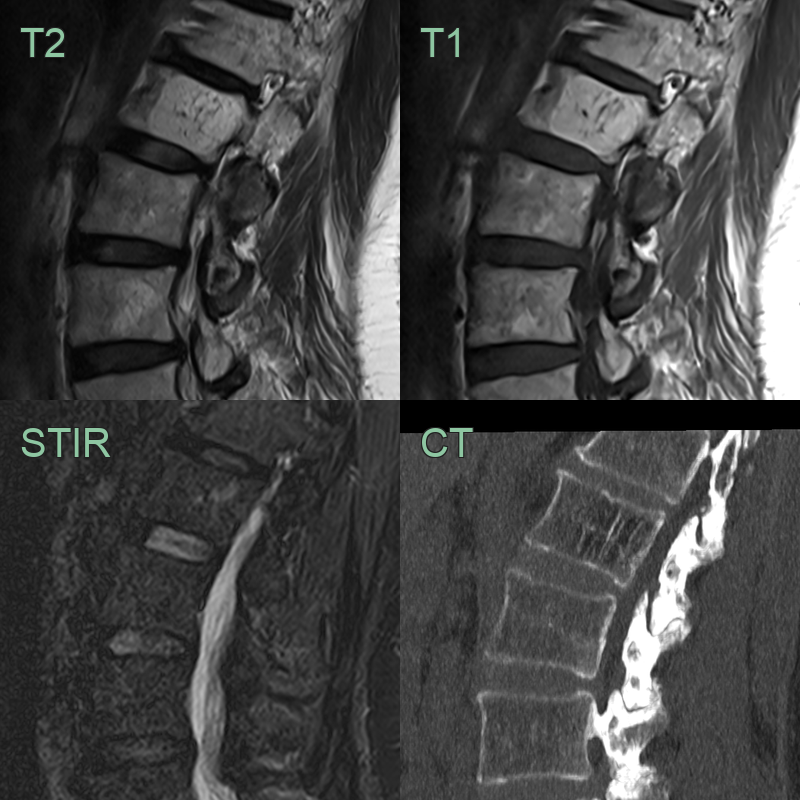
- An incidental finding in the L2 vertebral body was T1- and T2-hyperintense, due to fat content, and hypointense on STIR. CT showed the classical trabecular thickening of a hemangioma.
Treatment¶
- Almost always incidental and left alone. "Aggressive" hemangiomas (low fat, epidural extension, cord compression) may need embolisation, vertebroplasty, radiotherapy or surgery
- The T1-bright "polka-dot"/"corduroy" trabecular pattern is diagnostic
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Metastatic disease | Multiple lesions with destructive appearance; T1 hypointense and STIR hyperintense; no trabecular pattern |
| Multiple myeloma | Diffuse osteopenia; punched-out lytic lesions without sclerotic rim; no characteristic trabecular pattern |
| Lymphoma | Permeative pattern with soft tissue mass and epidural extension; no trabecular "polka-dot" appearance |
| Paget's disease | Coarsened trabecular pattern with bone enlargement and cortical thickening; "picture frame" appearance on plain film |
| Enostosis (bone island) | Smaller, dense sclerotic focus without trabecular pattern; no T2 signal change |
| Osteoblastoma | Expansile lytic lesion typically in posterior elements; variable enhancement; no trabecular pattern |
| Aneurysmal bone cyst | Multiple fluid-fluid levels on MRI; expansile thin-cortical shell; no trabecular pattern |
| Giant cell tumour | Eccentric location with soap-bubble appearance; extends to articular surface; no trabecular "corduroy" pattern |
| Osteoid osteoma | Small lesion with dense nidus and surrounding sclerosis; NaF PET avid; typically in posterior elements |
| Tuberculosis (Pott's disease) | Disc space involvement with end-plate erosion; paraspinal and psoas abscess; no preserved disc height |
-
Subramaniam et al. Management of Aggressive Vertebral Haemangioma and Assessment of Differentiating Pointers Between Aggressive Vertebral Haemangioma and Metastases - A Systematic Review. 2023. Global spine journal - Open in new tab. ↩