Acute Ischaemic Stroke¶
Summary
- Acute ischaemic stroke is characterised by sudden onset neurological deficits due to focal brain ischaemia
- Caused by thrombotic or embolic occlusion of cerebral arteries
- Rapid diagnosis and treatment are crucial for improved outcomes
Pathophysiology¶
- Arterial occlusion causes energy failure, ionic pump failure and excitotoxic cell death in the ischaemic core
- The surrounding penumbra is hypoperfused but potentially salvageable, and is lost progressively without reperfusion
Demographics¶
- Incidence rises steeply with age
- Modifiable risk factors: hypertension, diabetes, smoking, obesity and atrial fibrillation
Diagnosis¶
- Sudden focal deficits (hemiparesis, aphasia, visual loss, ataxia); severity graded by NIHSS
- Capillary glucose and ECG (for atrial fibrillation) at presentation
Imaging¶
- Non-contrast CT (first-line): excludes haemorrhage; early signs are loss of grey–white differentiation, cortical/insular ribbon effacement and the hyperdense vessel sign; scored with ASPECTS
- CT angiography: locates the occlusion and grades collaterals
- CT perfusion: core (reduced CBV/CBF) versus penumbra (raised Tmax/MTT with preserved CBV)
- MRI: DWI is most sensitive for acute infarct (high DWI, low ADC); DWI–FLAIR mismatch estimates lesion age; PWI–DWI mismatch defines penumbra
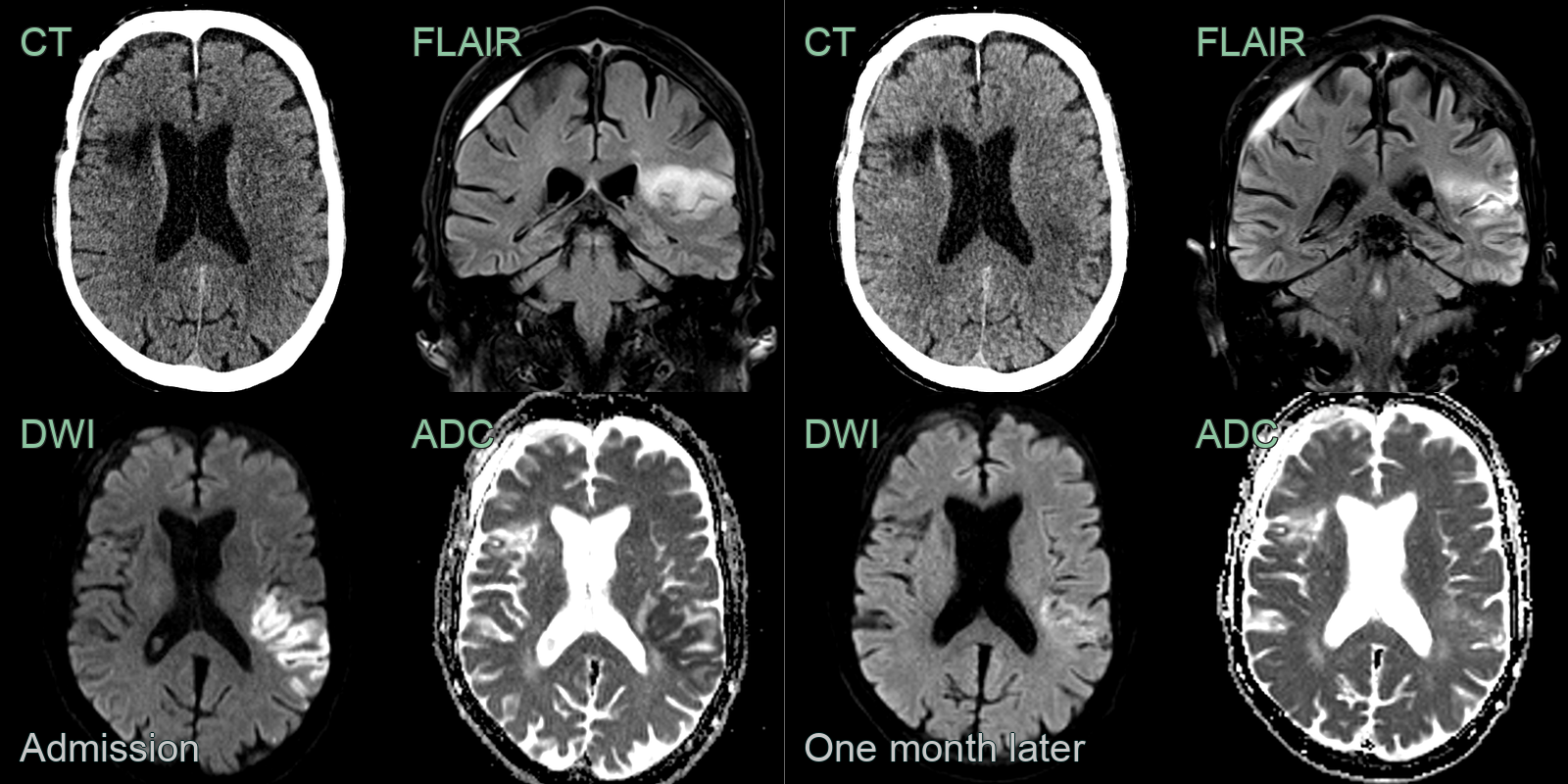
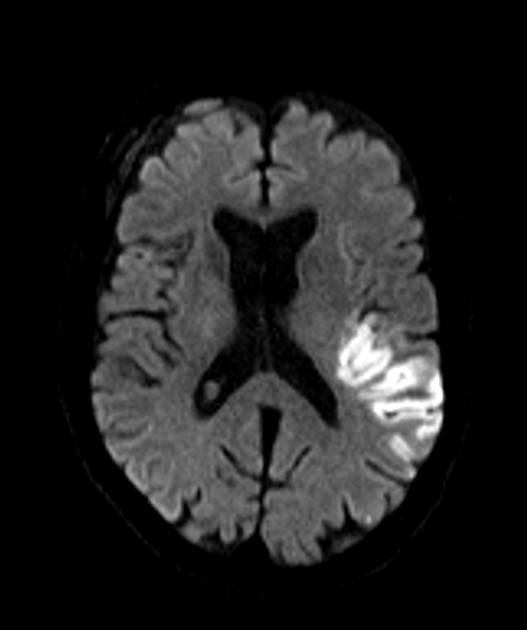
- A 70-year-old patient presenting with right sided weakness and dysarthria.
- At presentation, there was very subtle loss of grey-white matter differentiation on CT. On MRI, high DWI signal corresponded to low values on the ADC map.
- 1 month later, the DWI hyperintensity had regressed and the ADC values had increased.
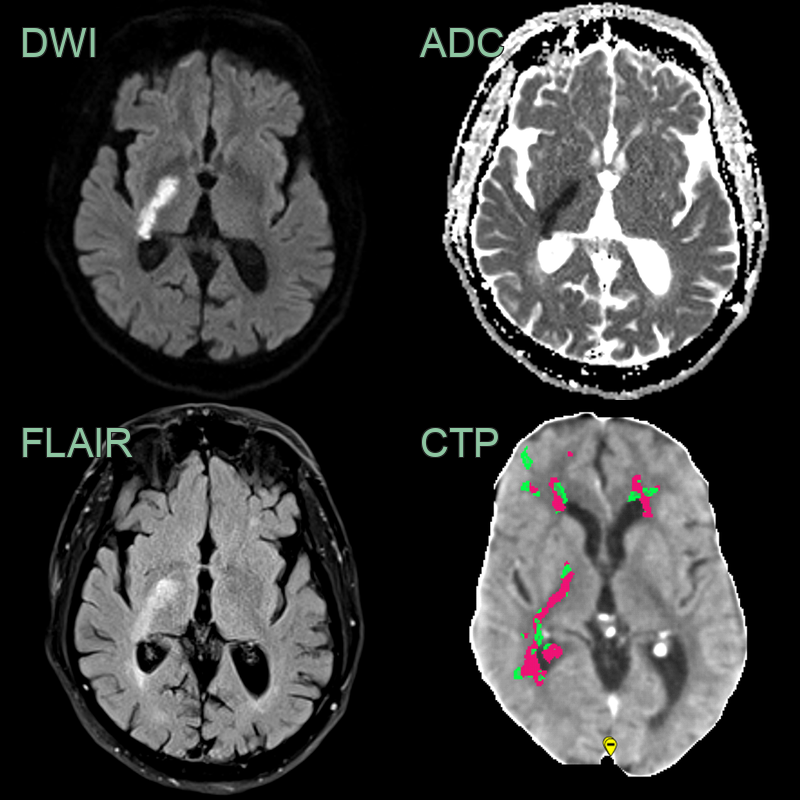
- A 65-year-old patient presenting with left sided weakness.
- DWI shows an acute infarct selectively involving the posterior limb of the internal capsule representing the territory of the anterior choroidal artery.
- While there was no abnormality on the CT, on hindsight, there was a region of abnormal perfusion (reduced CBF and increased Tmax) on the CTP performed the day prior.
- A 70-year-old patient present with a mixed sensory and motor deficit. While the NCCT did not convincing acute infarct, the CTA showed an area of hypoenhancement in the anterior thalamus. An acute thalamic infarct was confirmed on DWI.
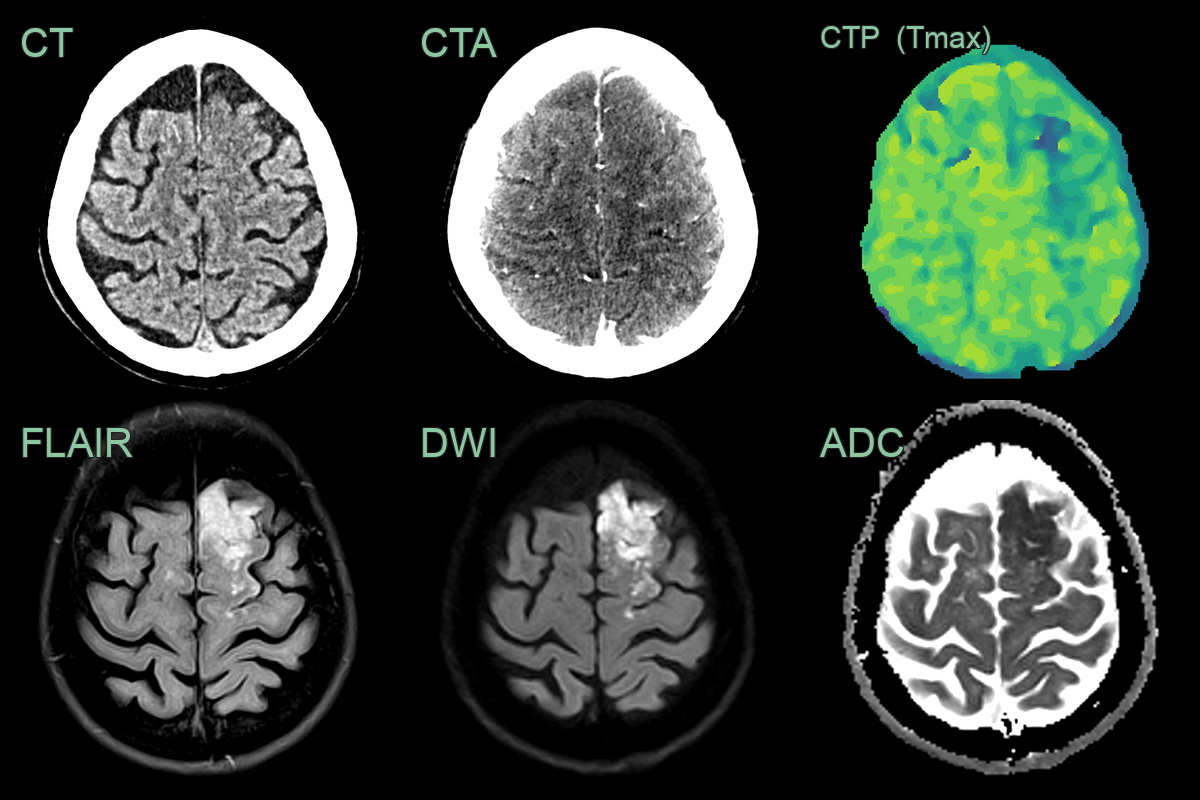
- A 60-year-old patient presented with aphasia and difficulty walking.
- CT showed a subtle region of cortical hypodensity in the left superior frontal gyrus (corresponding to the left ACA territory).
- CTA showed cortical hypoenhancement.
- CTP showed a prolonged Tmax (and decreased CBF and CBV).
- MRI showed high FLAIR signal and diffusion restriction (hyperintensity on B1000 DWI images corresponding to low values on the ADC map).
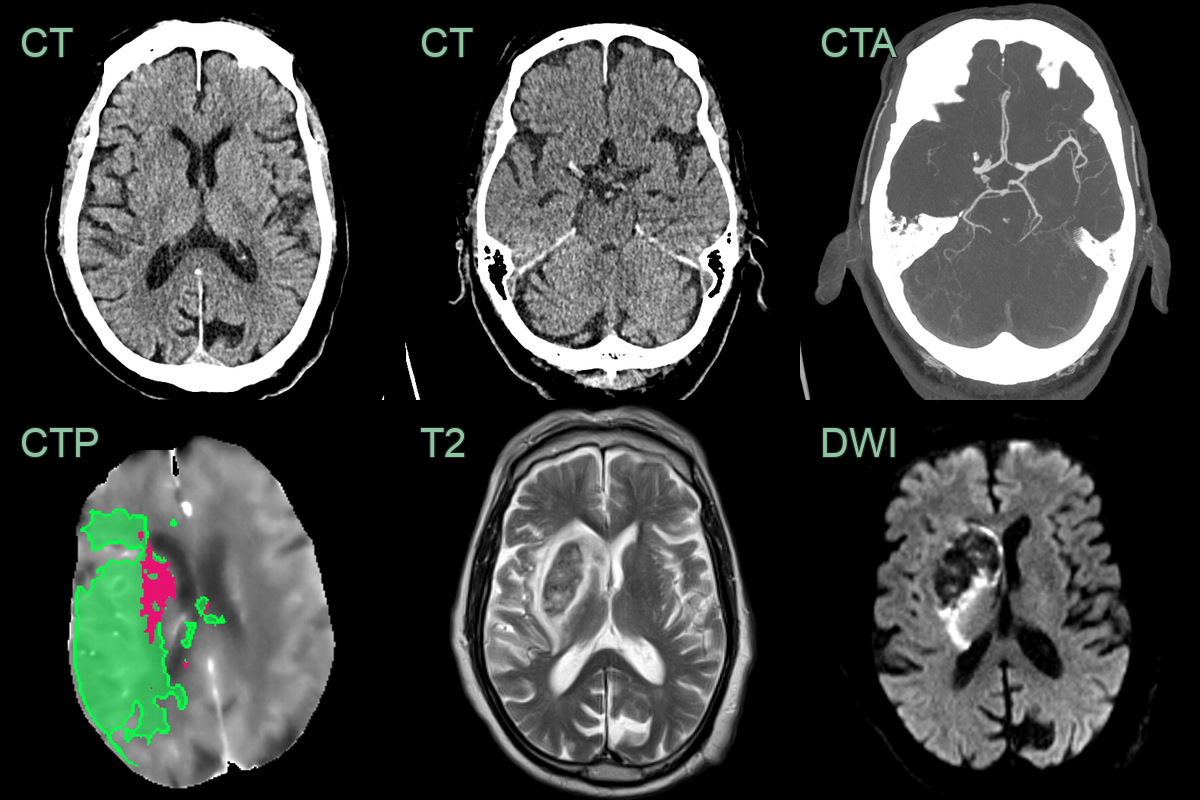
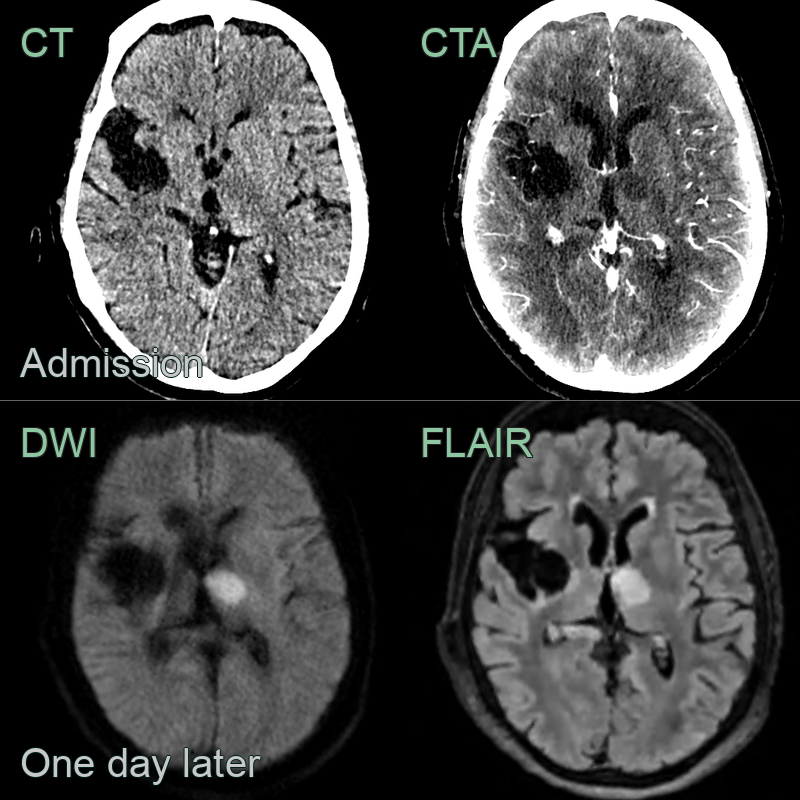
- A 80-year-old patient presented with a dense left sided weakness.
- CT showed a subtle area of acute ischaemia in the rigth caudate head.
- CTA showed a proximal occlusion of the right MCA.
- CTP showed a large penumbra and small core infarct.
- MRI performed 1 day after a mechnical thrombectomy showed no iscaehmic damage in the penumbra (and haemorrhagic transformation in the area of core infarction).
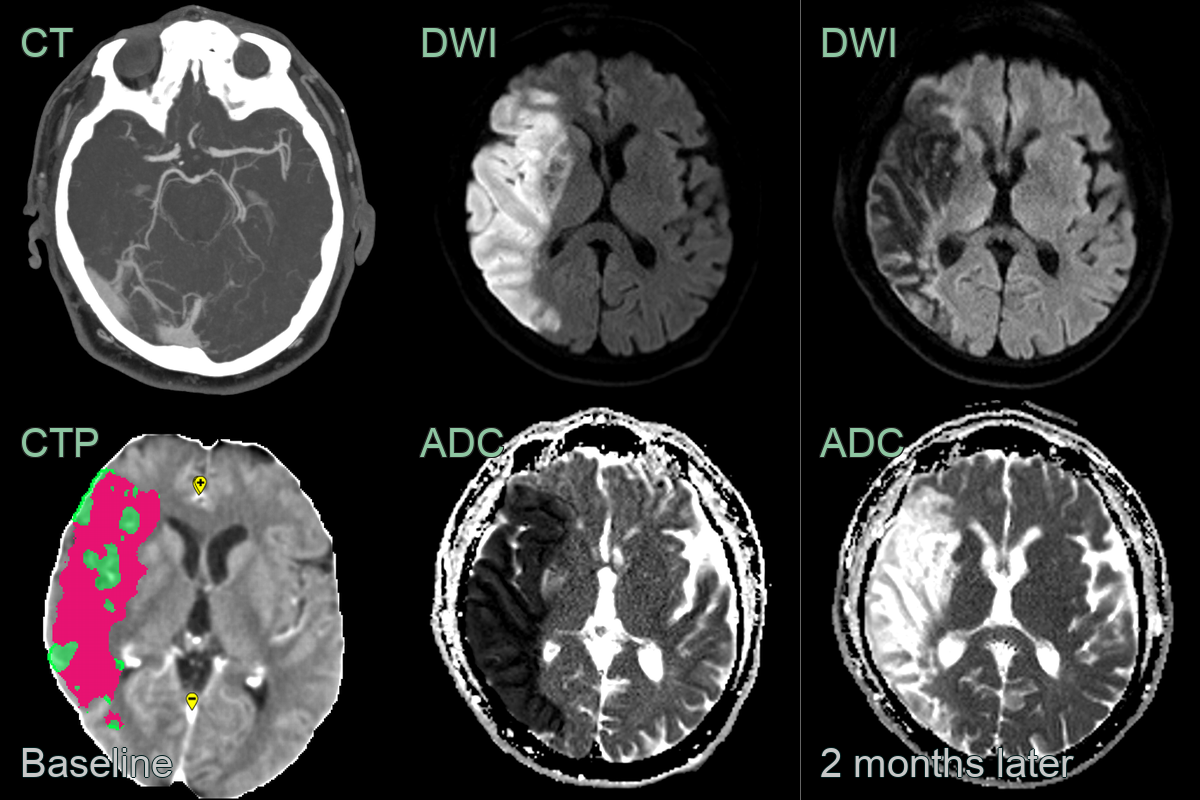
- A patient presented with a dense left sided hemiplegia.
- CTA showed a mid-M1 MCA occlusion. CTP showed a large core infarct (pink) with no sizeable penumbra (green).
- The diffusion restriction at baseline was replaced by facilitated diffusion due to encephalomalacia after 2 months.
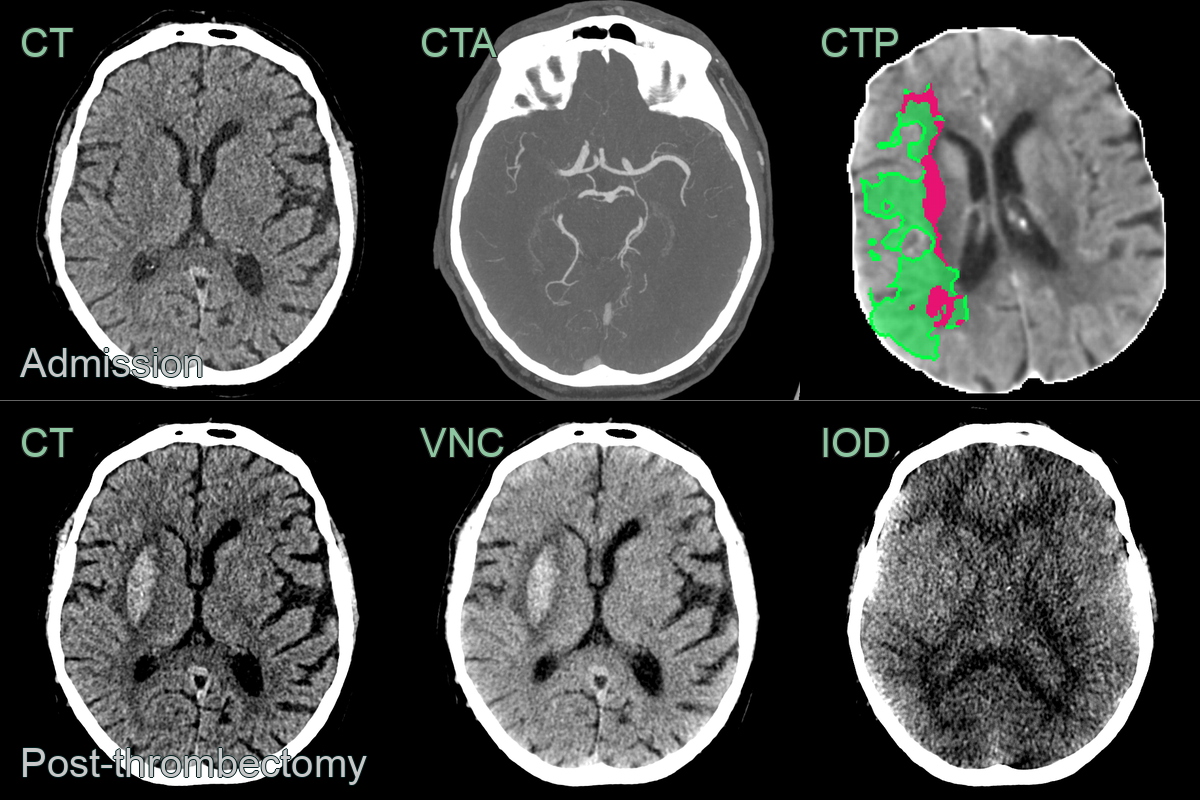
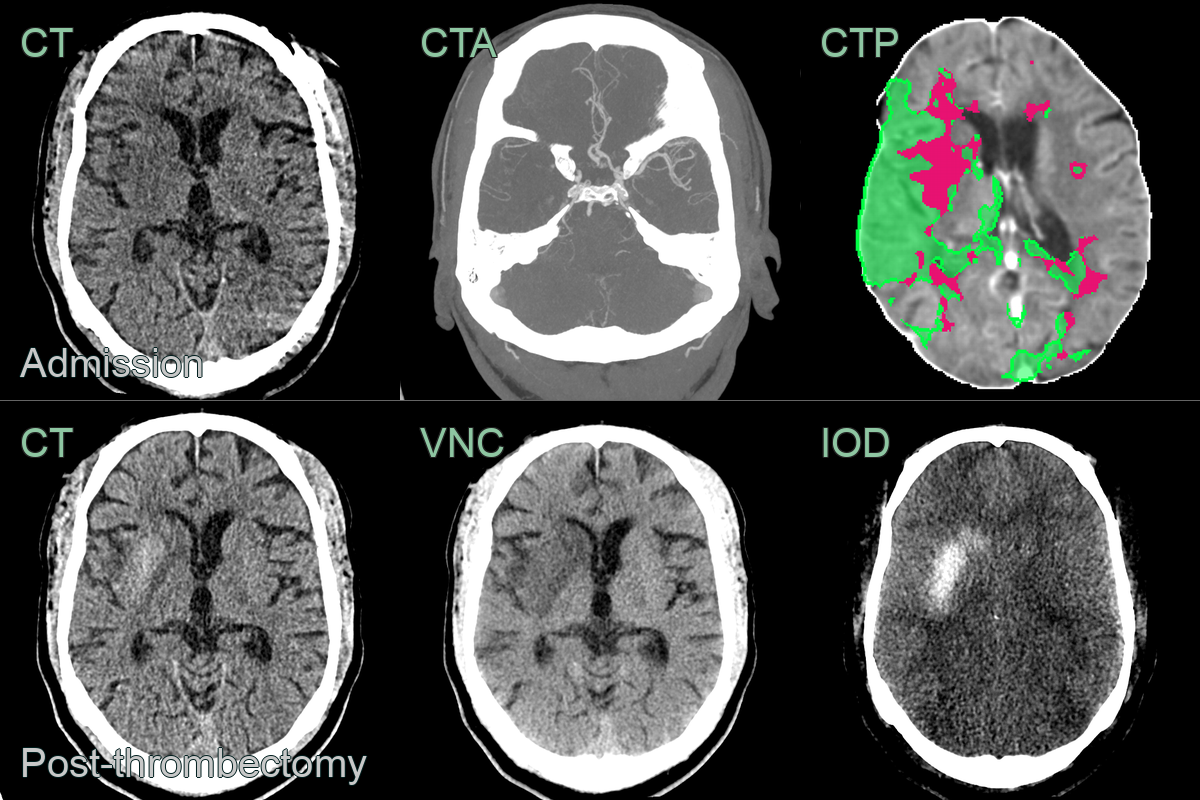
- A 70-year-old patient presented with a dense left-sided weakess.
- Imaging showed a right M1 MCA occlusion causing acute infarction (ASPECTS 8) associated with a large penumbra.
- Following a successful thrombectomy, the CT showed hyperdensity on CT. Using dual energy CT, the virtual non-contrast (VNC) showed hyperdensity in the right putamen that was not absent on the iodine map, consistent with petechial haemorrhage (as opposed to iodine staining where the inverse would have been true).
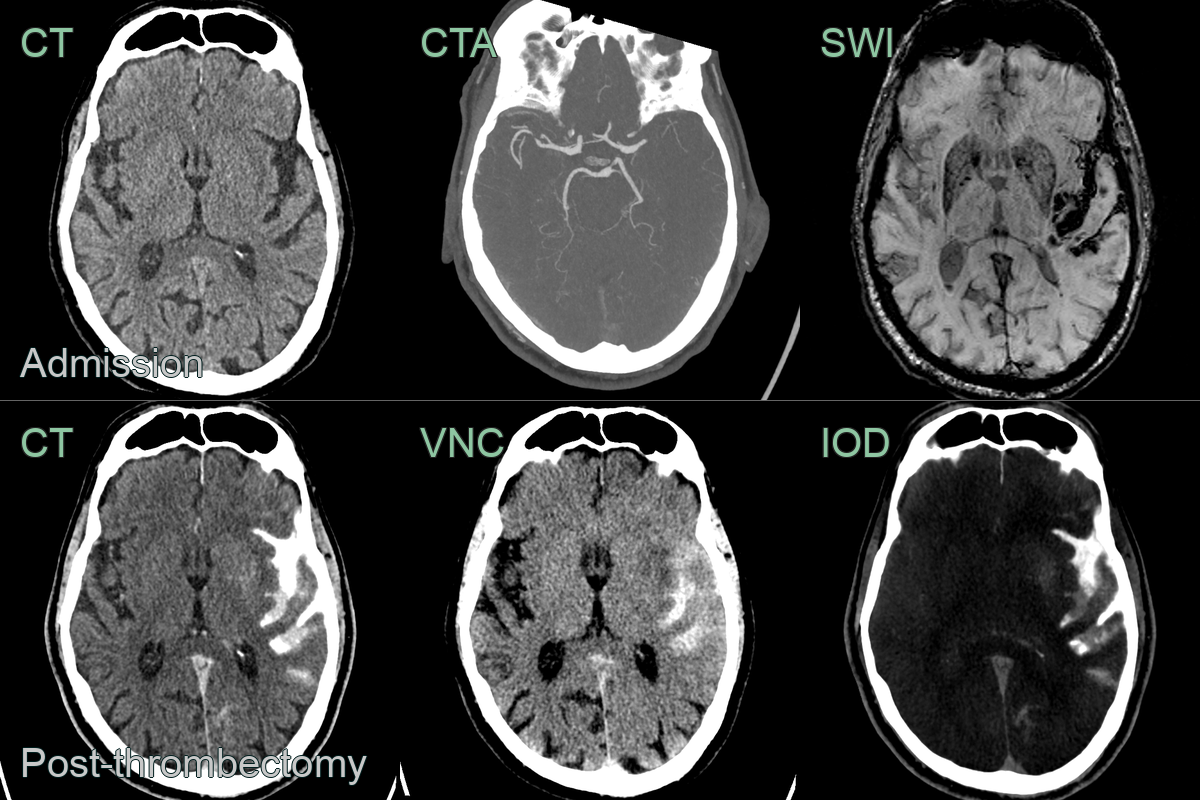
- A 50-year-old patient presented with left sided weakness secondary to a right M1 MCA occlusion.
- Contrary to the previous case, the hyperdensity in the right putamen was present on the iodine map but not the virtual non-contrast, which was consistent with iodine staining.
- A 65-year-old patient presented with dysphasia and right sided weakness secondary to an occluded left M1 MCA.
- Post-thrombectomy, high attenuation in the subarachnoid space was due to a combination of subarachnoid haemorrhage and seepage of iodinated contrast.
Treatment¶
- Intravenous thrombolysis within 4.5 hours (tenecteplase or alteplase)
- Mechanical thrombectomy for large-vessel occlusion, extendable to 24 hours in patients selected by clinical–core or perfusion mismatch1
- Secondary prevention: antiplatelet/anticoagulation, statin and risk-factor control
Differential diagnosis¶
| Differential Diagnosis | Distinguishing Feature |
|---|---|
| HSV encephalitis | May cross arterial territories |
-
Nogueira et al. Thrombectomy 6 to 24 Hours after Stroke with a Mismatch between Deficit and Infarct. 2018. The New England journal of medicine - Open in new tab. ↩