Arterial Dissection¶
Summary
- Arterial dissection is characterised by a tear in the intimal layer of an artery, allowing blood to enter the vessel wall and create a false lumen
- Common locations include carotid, vertebral, and aortic arteries
- Imaging plays a crucial role in diagnosis and management1
Pathophysiology¶
- Intimal tear allows blood to enter the media, creating a false lumen
- Propagation of dissection can lead to:
- Luminal narrowing or occlusion
- Aneurysmal dilatation
- Rupture
- Mechanisms:
- Spontaneous (e.g., connective tissue disorders)
- Traumatic (e.g., blunt or penetrating injury)
- Iatrogenic (e.g., catheterization procedures)
Demographics¶
- Incidence: 2.6-3.0 per 100,000 person-years for carotid dissection
- Age: Peak incidence in 40-50 years old
- Gender: Slight male predominance
- Risk factors:
- Hypertension
- Smoking
- Connective tissue disorders (e.g., Marfan syndrome, Ehlers-Danlos syndrome)
- Recent trauma or chiropractic manipulation
Diagnosis¶
- Clinical presentation:
- Headache or neck pain
- Neurological deficits (e.g., TIA, stroke)
- Horner's syndrome (in carotid dissection)
- Laboratory tests:
- D-dimer (elevated in acute dissection)
- Imaging:
- Essential for definitive diagnosis
Imaging¶
- CTA (first-line): tapered ("flame-shaped") stenosis or occlusion, intimal flap, double lumen, mural thrombus and any pseudoaneurysm
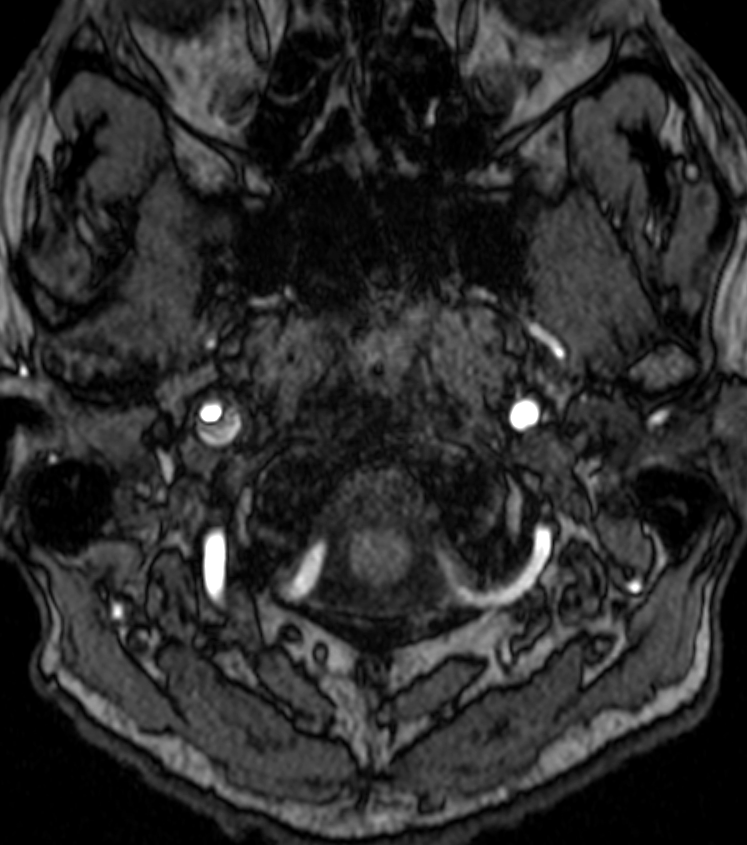
- MRI/MRA: the crescentic T1-hyperintense intramural haematoma on fat-saturated T1 is the most specific sign (subacute methaemoglobin); may show associated infarcts on DWI
- Ultrasound has a limited, mainly follow-up, role
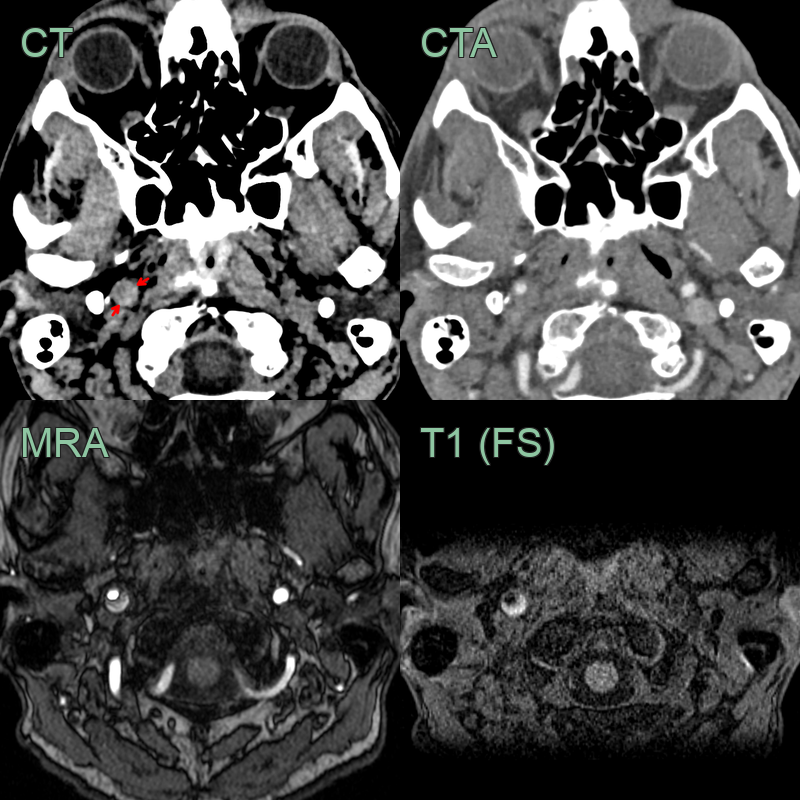
- Patient presented with a right sided Horner's syndrome after a falling of bicycle.
- NCCT showed an expanded right ICA jus below the skull base with a hyperdense rim.
- The lumen was not narrowed on CTA.
- T1-weighted imaging showed a crescent of high signal representing intramural haematoma.
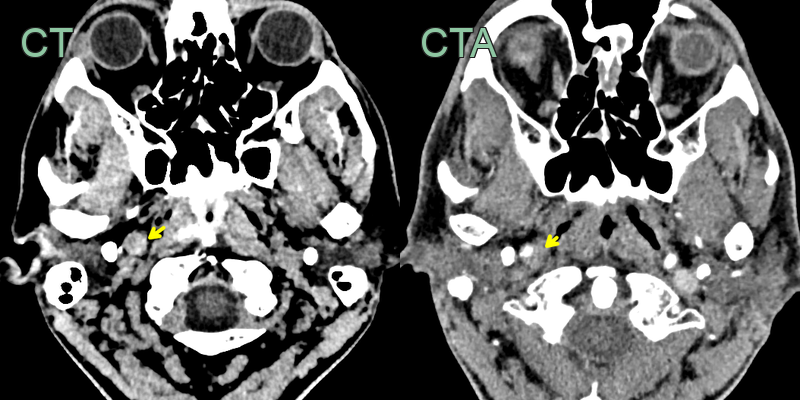
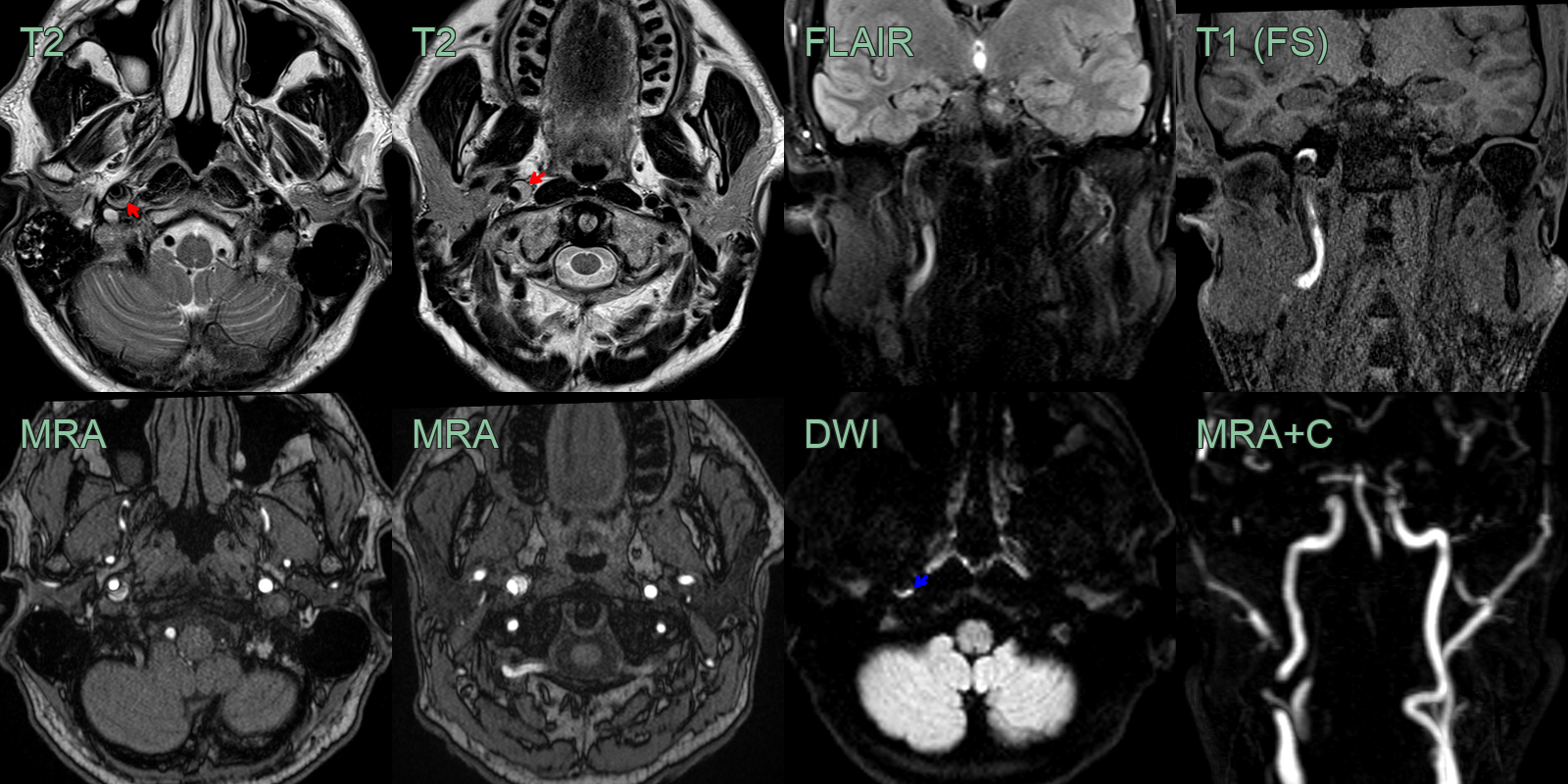
- 50-year-old patient presented with sudden onset right sided neck pain and a Horner's syndrome (blurred vision, right sided miosis and ptosis).
- The initial CT and CTA showed a hyperdense rim around an expanded right ICA below the skull base without a significant stenosis (yellow arrow).
- The T1-weighted imaging showed a T1-hyperintense rim around the ICA (red arrow).
- The mural thrombus also showed diffusion restriction (blue arrow) and blooming on SWI (not shown).
Treatment¶
- Antiplatelet or anticoagulation to prevent thromboembolic stroke
- Endovascular stenting/embolisation for flow-limiting dissection or symptomatic pseudoaneurysm
- Follow-up CTA/MRA at 3–6 months
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Atherosclerotic disease | Gradual onset, risk factors present, no intimal flap on imaging |
| Aneurysm | Focal dilatation, no intimal flap, often asymptomatic |
| Vasculitis | Vessel wall thickening and enhancement on high-resolution MRI; no crescentic intramural haematoma; multifocal involvement |
| Fibromuscular dysplasia | Beaded "string of beads" appearance on angiography; no intramural haematoma on fat-saturated T1 |
| Spontaneous intramural haematoma | Circumferential rather than eccentric wall thickening; no double lumen or intimal flap |
| Thromboembolism | No intramural haematoma on T1 fat-saturated; intraluminal filling defect rather than mural thickening |
| Pseudoaneurysm | Saccular outpouching at vessel wall; no crescentic T1 intramural signal |
-
Nash et al. Craniocervical Arterial Dissection in Children: Pathophysiology and Management. 2019. Pediatric neurology - Open in new tab. ↩