Atypical Teratoid/Rhabdoid Tumour (AT/RT)¶
Summary
- Rare, highly aggressive embryonal tumour of the central nervous system (CNS)
- Primarily affects young children, typically under 3 years of age
- Characterised by loss of INI1/SMARCB1 gene expression and distinctive imaging features1
Pathophysiology¶
- Arises from embryonal cells in the CNS
- Defined by biallelic inactivation of SMARCB1 gene (95% of cases) or SMARCA4 gene (2% of cases)
- Loss of these genes leads to dysregulation of chromatin remodelling and cell cycle control
- Histologically heterogeneous, containing rhabdoid cells, primitive neuroectodermal cells, and mesenchymal elements
Demographics¶
- Accounts for 1-2% of paediatric brain tumours
- Median age at diagnosis: 17 months
- Slight male predominance (1.6:1)
- Rare cases reported in adults
Diagnosis¶
- Clinical presentation:
- Rapid onset of neurological symptoms
- Increased intracranial pressure
- Focal neurological deficits
- Laboratory findings:
- CSF cytology may show malignant cells
- Histopathology:
- Characteristic loss of INI1/SMARCB1 protein expression on immunohistochemistry
- Presence of rhabdoid cells with eccentric nuclei and eosinophilic cytoplasmic inclusions
Imaging¶
- CT:
- Hyperdense, heterogeneous mass
- Often with areas of haemorrhage and necrosis
- Calcifications in 40-60% of cases
- MRI:
- T1: Heterogeneous, predominantly iso- to hypointense
- T2: Heterogeneous, predominantly hyperintense
- T1 post-contrast: Heterogeneous enhancement
- DWI: Restricted diffusion in solid components
- MR spectroscopy: Elevated choline, reduced NAA, presence of lipid/lactate peaks
- Location:
- 50-60% infratentorial (cerebellum, brainstem)
- 40-50% supratentorial
- Rarely in the spinal cord
- Distinctive features:
- "Cyst and nodule" appearance in some cases
- Frequent leptomeningeal dissemination at diagnosis (20-30%)
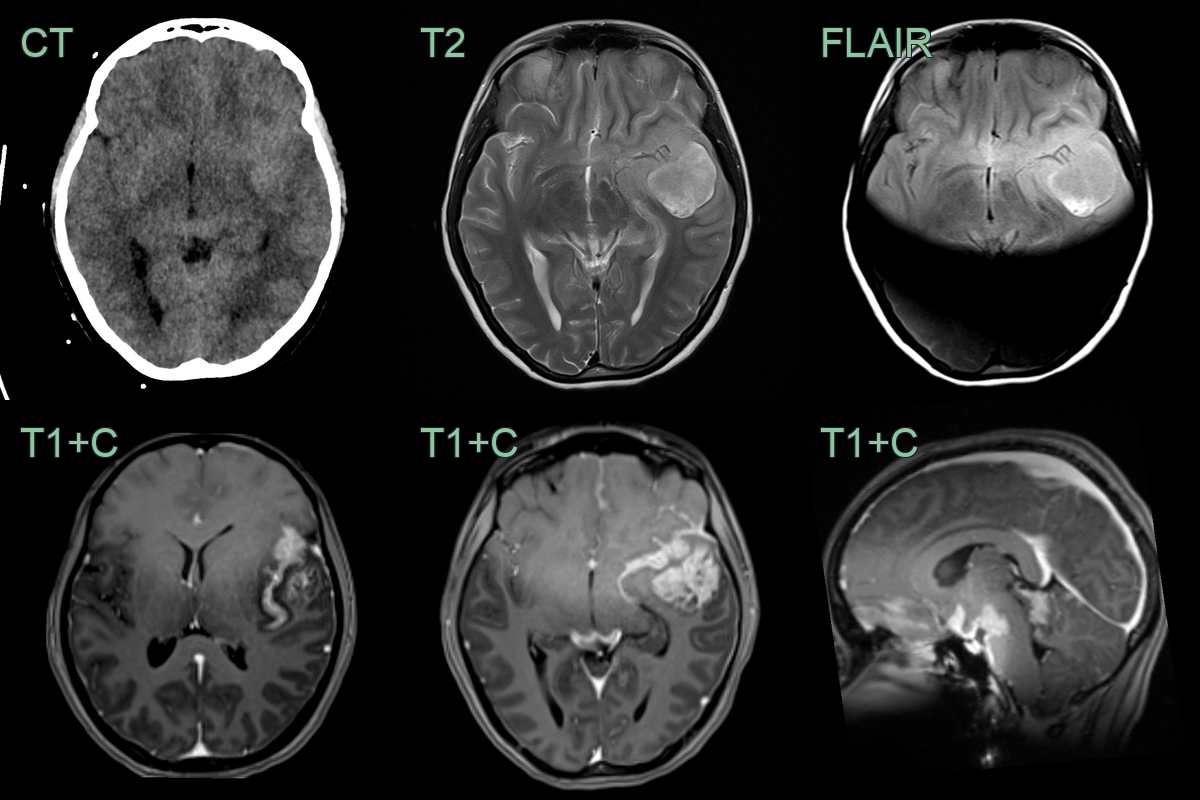
- A 15-year-old patient presenting with seizures and headache.
- CT showed only subtle hyperdensity in the left anterior temporal lobe and surrounding sulci.
- MRI showed an heterogeneously enhancing tumour in the left anterior frontal lobe with extensive leptomeningeal disease in the anterior, middle and posterior cranial fossae.
Treatment¶
- Multimodal: maximal safe resection, intensive chemotherapy and craniospinal irradiation (usually deferred in children under 3)
- Prognosis is poor, though better with older age, gross total resection and localised disease
Differential diagnosis¶
| Imaging differential | Differentiating feature |
|---|---|
| Medulloblastoma | Midline fourth-ventricular mass, more homogeneous with uniform restricted diffusion; AT/RT is more often off-midline/CPA and heterogeneous with haemorrhage |
| Ependymoma | "Plastic" tumour extruding through the fourth-ventricular outlets; less haemorrhage |
| Choroid plexus carcinoma | Avidly enhancing intraventricular frond-like mass with brain invasion |
| Embryonal tumour with multilayered rosettes (ETMR) | Large, bulky supratentorial mass; overlapping imaging, distinguished by C19MC amplification |
| Pilocytic astrocytoma | Cyst-with-enhancing-nodule, facilitated (not restricted) diffusion |
-
Richardson et al. Atypical Teratoid Rhabdoid Tumour : From Tumours to Therapies. 2018. Journal of Korean Neurosurgical Society - Open in new tab. ↩