Pilocytic Astrocytoma (PCA)¶
Summary
- Pilocytic astrocytoma is a slow-growing, WHO grade 1 glial tumour typically affecting children and young adults
- Characterised by biphasic histology with compact bipolar cells and loose-textured multipolar cells
- Imaging features include cystic components with an enhancing mural nodule, most commonly in the cerebellum1
Pathophysiology¶
- Arises from astrocytes, a type of glial cell in the central nervous system
- Typically associated with alterations in the MAPK pathway
- BRAF-KIAA1549 fusion gene is the most common genetic alteration (found in 60-80% of cases)
- BRAF V600E mutation occurs in a minority of cases
- Slow-growing tumour with limited infiltrative potential
- Often well-circumscribed with a tendency to form cysts
Demographics¶
- Most common primary brain tumour in children
- Peak incidence between 5-15 years of age
- Slight male predominance (M:F ratio 1.2:1)
- Accounts for approximately 15% of all brain tumours in children
- Can occur in adults but less common
Diagnosis¶
- Clinical presentation varies depending on tumour location:
- Cerebellar lesions: ataxia, headache, nausea, vomiting
- Optic pathway lesions: visual disturbances, proptosis
- Brainstem lesions: cranial nerve palsies, long tract signs
- Histopathology:
- Biphasic pattern with compact bipolar cells (piloid) and loose-textured multipolar cells
- Rosenthal fibres and eosinophilic granular bodies often present
- Low mitotic activity and absence of necrosis
- Immunohistochemistry:
- GFAP positive
- Ki-67 proliferation index typically low (<1%)
Imaging¶
- CT:
- Well-circumscribed, hypodense cystic mass with an isodense to hyperdense mural nodule
- Calcification uncommon (10-20% of cases)
- MRI:
- T1: cystic component hypointense, solid component isointense to grey matter
- T2/FLAIR: cystic component hyperintense, solid component heterogeneous but predominantly hyperintense
- T1 post-contrast: intense enhancement of solid component and cyst wall
- DWI: typically no restricted diffusion
- MR spectroscopy: elevated choline, decreased NAA, absence of lipid/lactate peak
- Common locations:
- Cerebellum (60%)
- Optic pathway/hypothalamus (20%)
- Brainstem (10%)
- Cerebral hemispheres (10%)
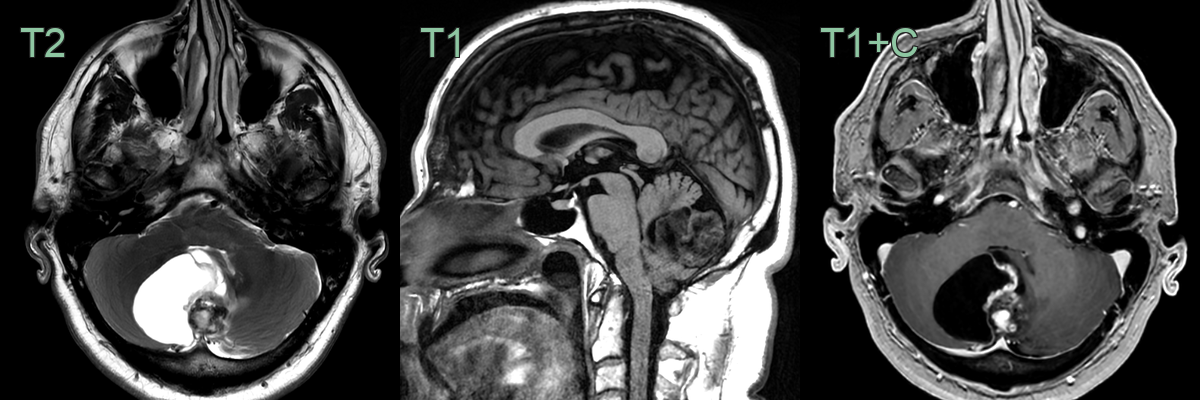
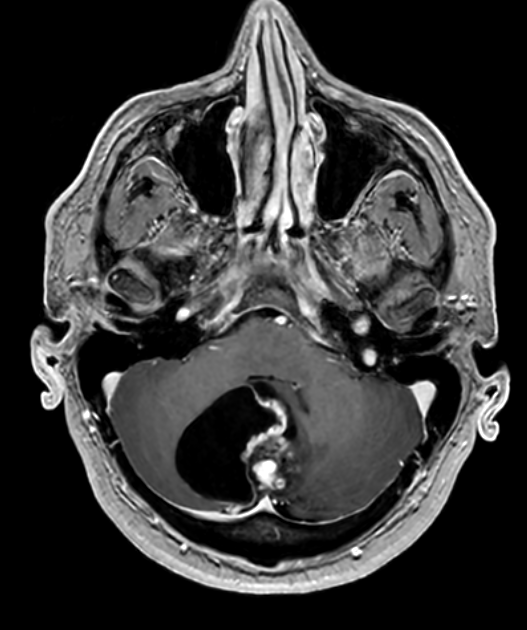
- 50-year-old patient presented with neck stiffness and imbalance.
- MRI showed a solid-cystic cerebellar lesion with heterogeneous enhancement.
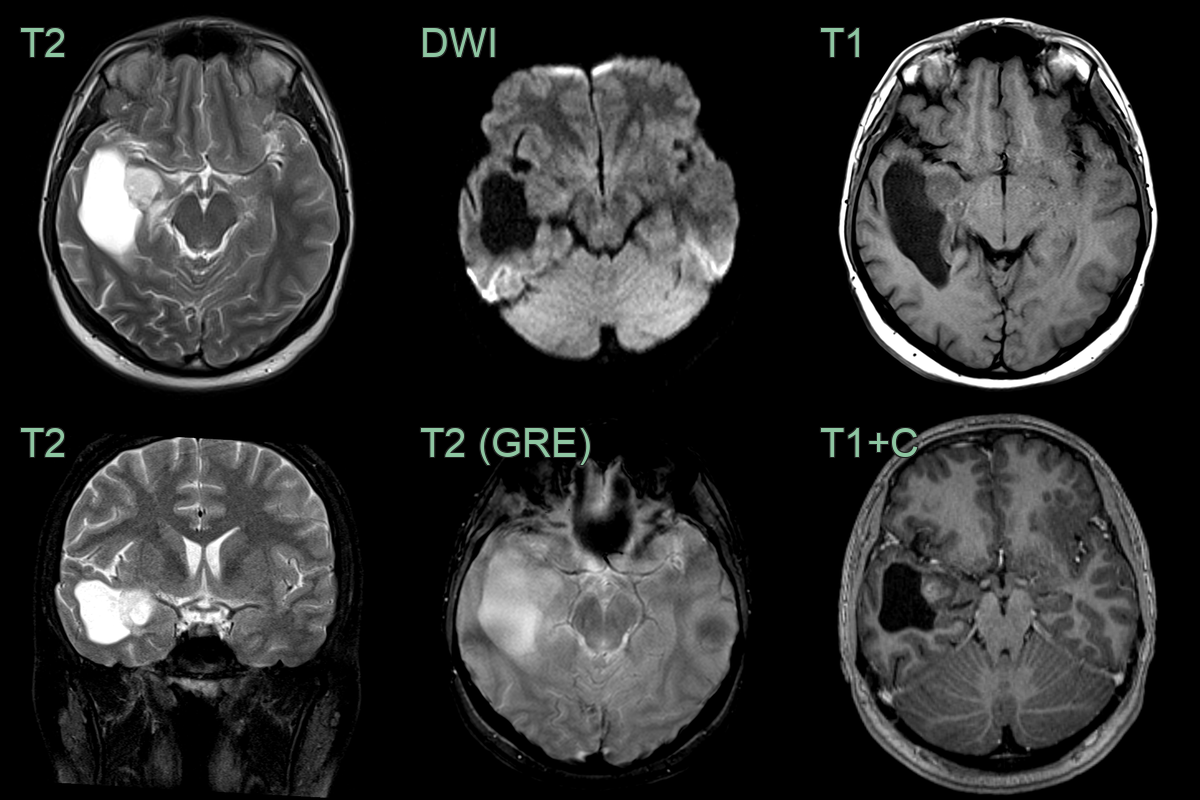
- 18-year-old patient presented after a seizure.
- MRI showed a solid-cystic lesion with no diffusion restriction or haemorrhage in the right mesial temporal lobe.
Treatment¶
- Complete resection is usually curative; MAPK-pathway inhibitors (BRAF/MEK) for unresectable or recurrent disease. The cyst-with-enhancing-mural-nodule in the cerebellum is the classic appearance
Differential diagnosis¶
| Differential Diagnosis | Distinguishing Feature |
|---|---|
| Ependymoma | Typically intraventricular; PCA is usually extra-ventricular |
| Medulloblastoma | Typically in cerebellar vermis; PCA more often in cerebellar hemispheres |
| Ganglioglioma | Often has calcifications; PCA rarely calcifies |
| Hemangioblastoma | Smaller enhancing mural nodule with angiographic blush; cyst wall does not enhance; associated with von Hippel-Lindau in younger patients |
| Low-grade glioma | Typically infiltrative without cystic component; no discrete mural nodule; T2/FLAIR mismatch sign |
| Dysembryoplastic neuroepithelial tumour (DNET) | Cortical location; PCA is typically deep-seated |
| Pleomorphic xanthoastrocytoma | Superficial cerebral location; PCA is often in cerebellum or optic pathway |
| Oligodendroglioma | Typically in cerebral hemispheres; PCA rare in this location |
| Abscess | Ring-enhancing with restricted diffusion within the cavity; surrounding oedema; no mural nodule |
-
Salles et al. Pilocytic Astrocytoma: A Review of General, Clinical, and Molecular Characteristics. 2020. Journal of child neurology - Open in new tab. ↩