Oligodendroglioma¶
Summary
- Oligodendroglioma is a slow-growing, diffusely infiltrating glial tumour of the central nervous system
- Typically affects adults in their 4th-5th decades of life
- Characterised by classic "fried egg" appearance histologically and 1p/19q co-deletion genetically1
Pathophysiology¶
- Typically occurs in the cerebral hemispheres, particularly the frontal lobes
- Molecular markers include 1p and 19q co-deletion and IDH½ mutation
- Typical findings of histopathological include "fried egg" oligodendrocytes, chicken-wire neovascularisation and microcalcification
Demographics¶
- Accounts for approximately 5-20% of all gliomas and 5-10% of all intracranial tumours
- Peak incidence in 4th-5th decades of life
- Slight male predominance (M:F ratio 1.1-2:1)
Diagnosis¶
- Clinical presentation:
- Seizures (50-80% of cases)
- Headaches
- Focal neurological deficits
- Cognitive changes
Imaging¶
- CT:
- Hypoattenuating cortical/subcortical mass
- Calcifications in 50-90% of cases
- May cause remodelling of the overlying skull (representing slow growth)
- MRI:
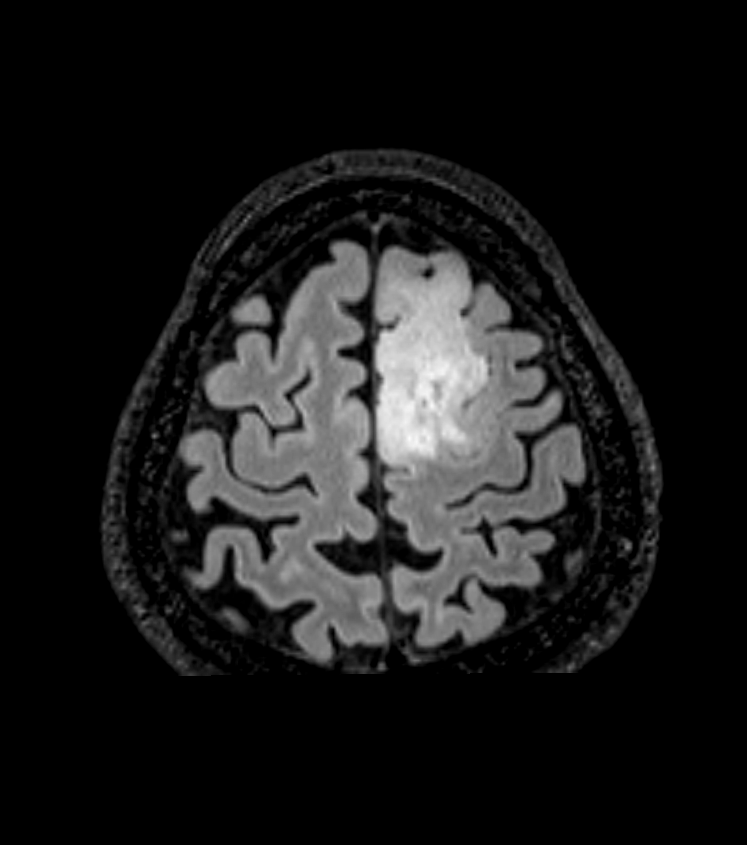
- ++T2/FLAIR++ hyperintense
- ++T1++ hypointense to isointense
- ++T1C++ Minimal to moderate enhancement with contrast
- ++SWI++ Hypointensity/blooming due to calcification (or, more rarely, haemorrhage)
- Advanced imaging:
- MR spectroscopy: elevated Cho/NAA ratio, presence of lactate/lipid peak
- Perfusion imaging: CBV may be elevated even in grade 2 lesions
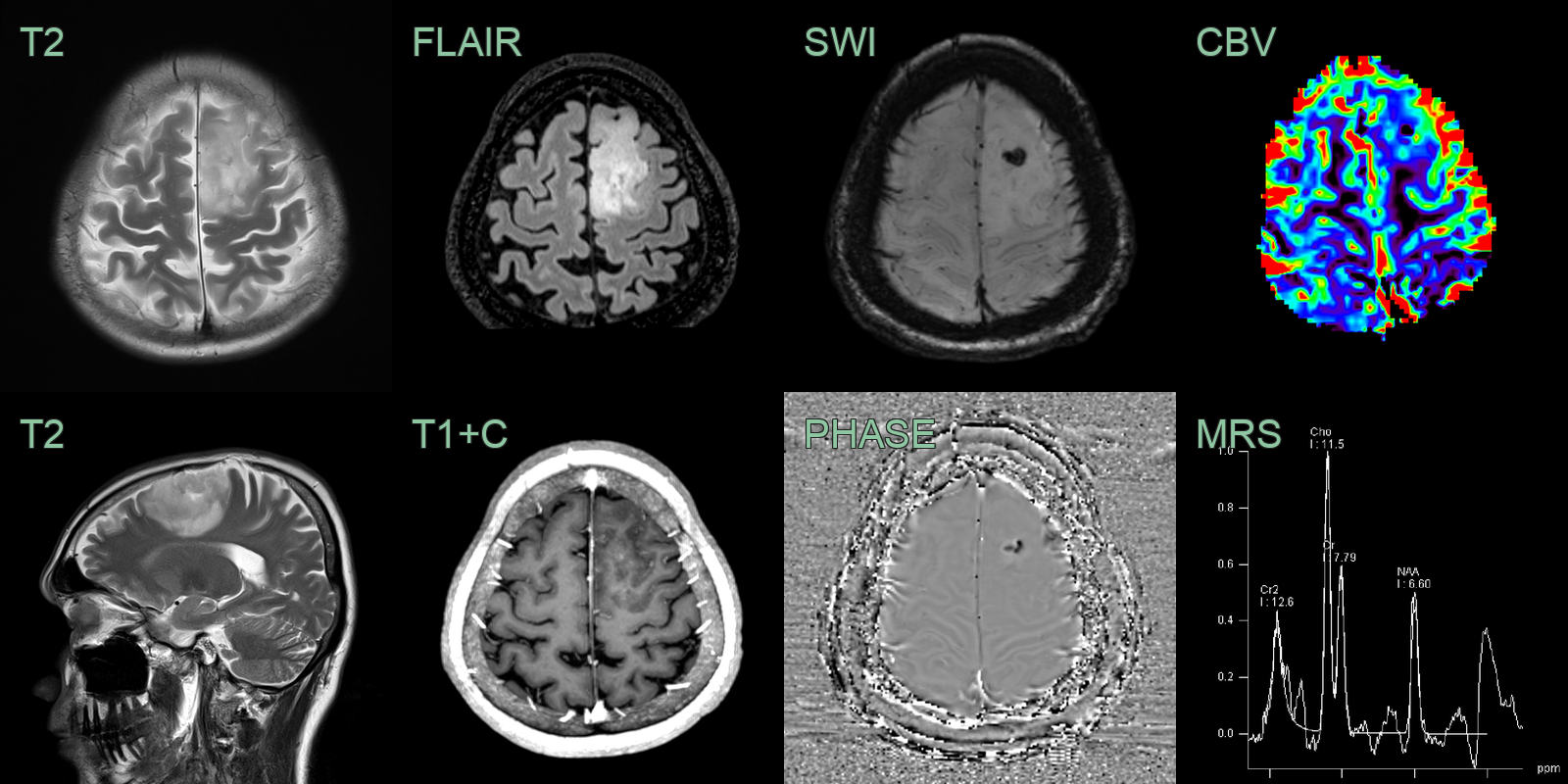
- A 40-year-old patient presented after a tonic-clonic seizure.
- MRI showed a relatively well-demarcated tumour in the left frontal lobe that involved cortex.
- Phase data from SWI showed diamagnetic susceptibility artefact consistent with dystrophic calcification.
- There was punctate enhancement and elevated CBV (ratio of 2.5 relative to contralateral normal-appearing brain tissue).
- MRS showed elevated choline and reduced NAA (indicating the replacement of normal neurons with mitotically active cells).
Treatment¶
- Maximal safe resection with radiotherapy and PCV chemotherapy for higher grade/risk
- Defined by IDH mutation and 1p/19q codeletion (both required); this confers a better prognosis and chemosensitivity than astrocytoma
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Astrocytoma | T2/FLAIR mismatch sign (bright T2 but suppressed on FLAIR) favours astrocytoma; less well-defined margins; calcification rare |
| Dysembryoplastic neuroepithelial tumour (DNET) | "Bubbly" multinodular cortical architecture; no enhancement; typically in younger patients |
| Ganglioglioma | Cystic lesion with mural nodule; mixed cystic-solid architecture; calcification less prominent |
| Glioblastoma | Central necrosis; ring enhancement; elevated rCBV; marked DWI restriction |
-
M Smits. Imaging of oligodendroglioma. 2016. The British journal of radiology - Open in new tab. ↩