Dysembryoplastic Neuroepithelial Tumour (DNET)¶
Summary
- Benign, slow-growing glioneuronal tumour typically presenting with drug-resistant epilepsy in children and young adults
- Characterised by cortical location, multinodular architecture, and specific glioneuronal element
- Imaging shows a cortical-based, multicystic lesion with minimal or no enhancement1
Pathophysiology¶
- Arises from abnormal development of neuroepithelial cells during embryogenesis
- Composed of oligodendrocyte-like cells, astrocytes, and floating neurons
- Typically lacks mitotic activity and necrosis
- Associated with cortical dysplasia in up to 80% of cases
Demographics¶
- Most common in children and young adults
- Mean age at diagnosis: 14-18 years
- Slight male predominance (male:female ratio 1.2:1)
- Accounts for 0.2-0.8% of all intracranial neoplasms
Diagnosis¶
- Clinical presentation:
- Drug-resistant focal epilepsy (>90% of cases)
- Seizure onset typically in childhood or adolescence
- Normal neurological examination in most patients
- Histopathology:
- WHO grade 1 tumour
- Specific glioneuronal element: oligodendrocyte-like cells arranged in columns
- Floating neurons in a mucoid matrix
- Immunohistochemistry: CD34 positivity in oligodendrocyte-like cells
Imaging¶
- CT:
- Hypodense cortical-based lesion
- Calcifications in 20-30% of cases
- MRI:
- T1: Hypointense to grey matter
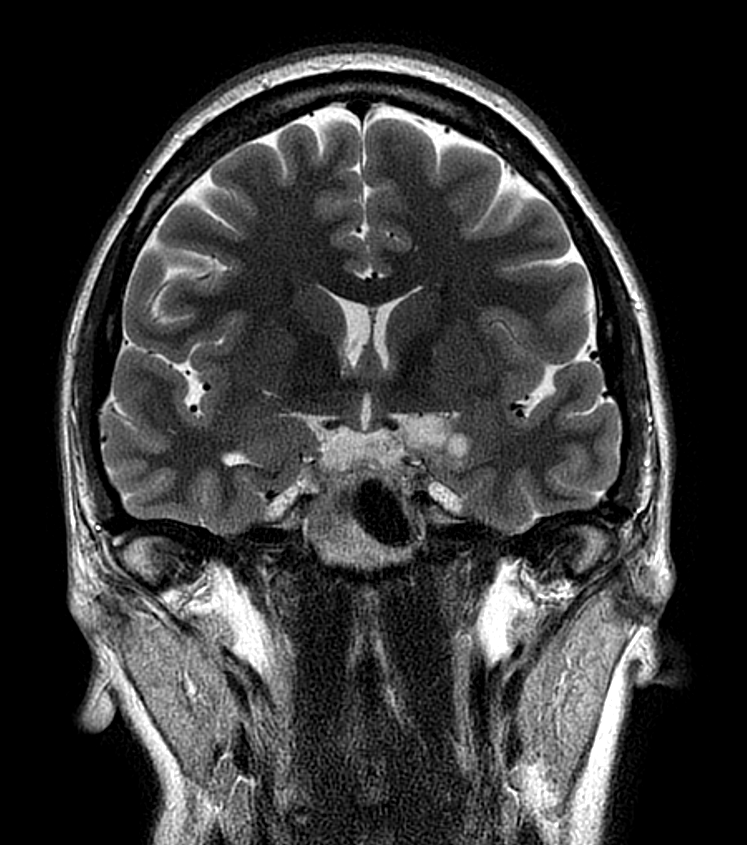
- T2/FLAIR: Hyperintense, multicystic appearance ("bubbly" or "soap bubble" appearance)
- Minimal or no enhancement after gadolinium administration
- No perilesional oedema
- "Bright rim sign": T2 hyperintense rim at the tumour-cortex interface (specific for DNET)
- Advanced imaging:
- MR spectroscopy: Reduced N-acetylaspartate, elevated myoinositol
- Perfusion imaging: Low relative cerebral blood volume
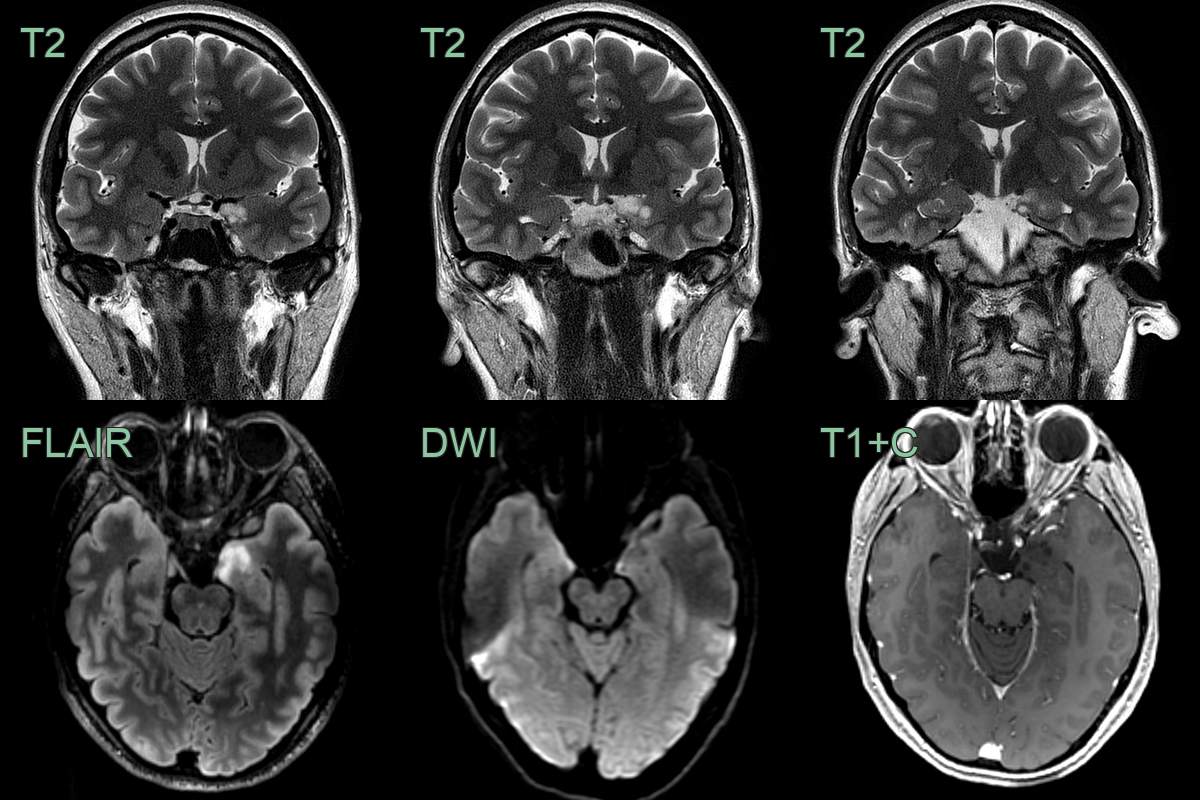
- Soap-bubble non-enhancing lesion in the left uncus has not changed in over 6 years giving a radiological diagnosis of DNET.
Treatment¶
- Surgical resection is curative and usually achieves seizure freedom; the lesion is stable if managed conservatively
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Low-grade glioma | DNETs have a characteristic "bubbly" appearance on T2-weighted MRI, while low-grade gliomas typically appear more homogeneous |
| Ganglioglioma | DNETs lack the calcifications often seen in gangliogliomas on CT scans |
| Focal cortical dysplasia | DNETs have a well-defined border, while focal cortical dysplasia often has blurred gray-white matter junction |
| Oligodendroglioma | DNETs are typically located in the temporal lobe, while oligodendrogliomas are more common in the frontal lobes |
| Pleomorphic xanthoastrocytoma | DNETs do not enhance with contrast, unlike pleomorphic xanthoastrocytomas which often show strong enhancement |
| Pilocytic astrocytoma | DNETs are typically cortical, while pilocytic astrocytomas are often found in the cerebellum or optic pathways |
| Cavernous malformation | DNETs lack the characteristic "popcorn" appearance and haemosiderin rim seen in cavernous malformations on MRI |
| Glioneural tumours | DNETs have a specific "floating neuron" histological pattern, which is absent in other glioneural tumours |
| Encephalocele | DNETs do not show direct communication with the subarachnoid space, unlike encephaloceles |
| Cortical tuber (in tuberous sclerosis) | DNETs are solitary lesions, while cortical tubers are typically multiple |
-
Raymond et al. Abnormalities of gyration, heterotopias, tuberous sclerosis, focal cortical dysplasia, microdysgenesis, dysembryoplastic neuroepithelial tumour and dysgenesis of the archicortex in epilepsy. Clinical, EEG and neuroimaging features in 100 adult patients. 1995. Brain : a journal of neurology - Open in new tab. ↩