Low Grade Glioma¶
Summary
- Low-grade gliomas (LGGs) are slow-growing primary brain tumours originating from glial cells
- Typically affect young adults and present with seizures or subtle neurological deficits
- Characterised by diffuse infiltration on imaging and require long-term follow-up due to potential for malignant transformation1
Pathophysiology¶
- Arise from glial cells (astrocytes, oligodendrocytes, or mixed)
- Under WHO 2021, adult-type grade 2 diffuse gliomas are astrocytoma (IDH-mutant) or oligodendroglioma (IDH-mutant, 1p/19q-codeleted); "oligoastrocytoma" is no longer used
- IDH mutation is near-universal; 1p/19q codeletion defines oligodendroglioma, ATRX loss defines astrocytoma
- Slow growth rate but infiltrative nature
Demographics¶
- Peak incidence: 30-40 years of age
- Slight male predominance (M:F ratio 1.3:1)
- Accounts for approximately 15% of all primary brain tumours
- More common in Caucasians compared to other racial groups
Diagnosis¶
- Clinical presentation:
- Seizures (most common initial symptom, 80-90% of cases)
- Headaches
- Subtle neurological deficits
- Cognitive changes
- Neurological examination may be normal or show mild focal deficits
- Neuropsychological testing may reveal cognitive impairments
- Definitive diagnosis requires histopathological examination and molecular testing
Imaging¶
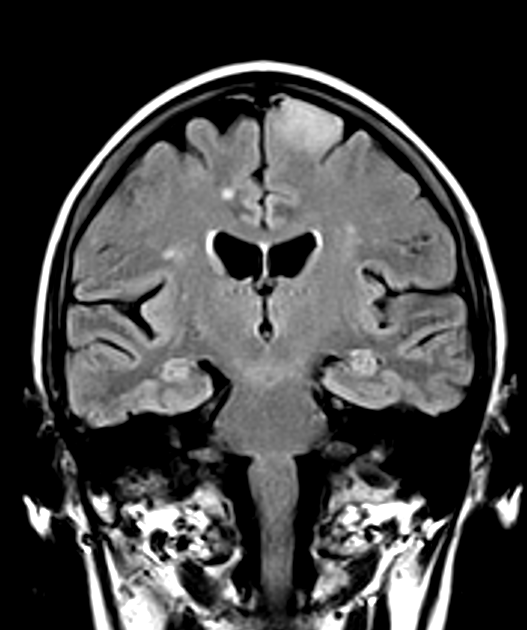
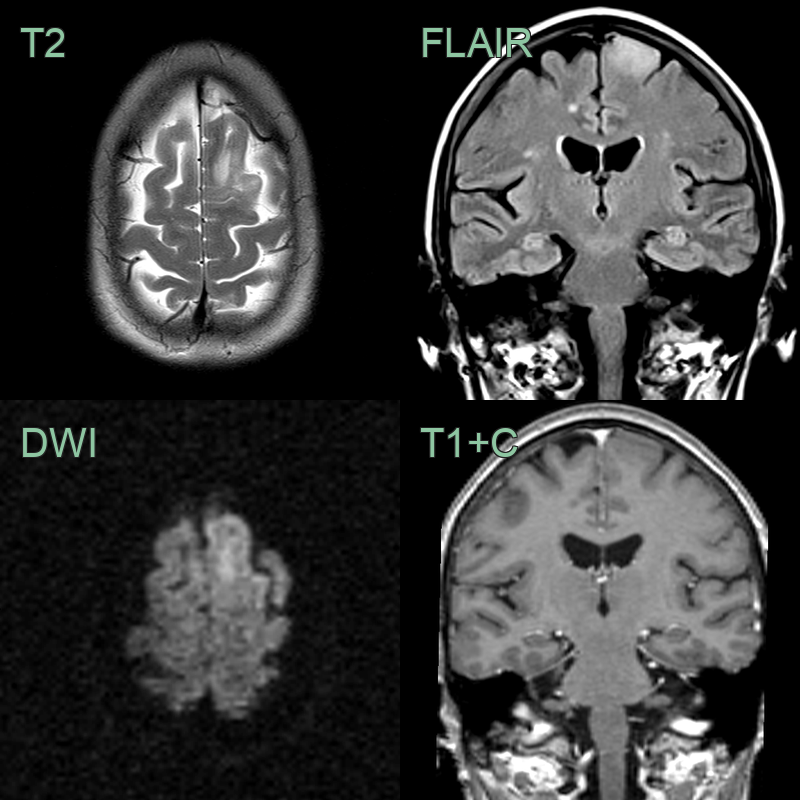
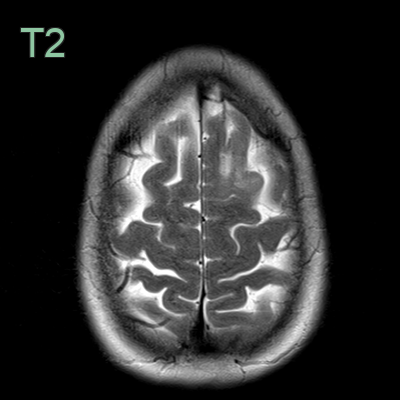
- MRI is the imaging modality of choice:
- T1-weighted: hypointense to isointense
- T2-weighted/FLAIR: hyperintense
- Minimal or no enhancement on post-contrast T1
- Diffusion restriction typically absent
- Advanced MRI techniques:
- Perfusion imaging: usually shows no increased cerebral blood volume
- MR spectroscopy: elevated Cho/NAA ratio, reduced NAA peak
- PET imaging:
- Hypometabolism on FDG-PET
- Increased uptake on amino acid PET (e.g., 11C-methionine)
Treatment¶
- Maximal safe resection, with radiotherapy/chemotherapy (PCV or temozolomide) for higher-risk disease
- IDH inhibitors (vorasidenib) are an emerging option; long-term surveillance is needed for malignant transformation
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Multiple sclerosis | Multiple ovoid periventricular lesions; calloso-septal interface; Dawson's fingers on sagittal FLAIR |
| Brain abscess | Ring enhancement with smooth thin capsule; restricted central DWI; surrounding vasogenic oedema |
| Metastasis | Multiple lesions at grey-white junction; surrounding vasogenic oedema disproportionate to size; nodular or ring enhancement |
| Subacute infarct | Follows vascular territory; wedge-shaped; cortical gyral enhancement; resolves on follow-up |
| Primary CNS lymphoma | Homogeneous enhancement; periventricular; restricted DWI; hyperdense on non-contrast CT |
| Encephalitis | Cortical/limbic T2 signal; temporal lobe predilection; may show restricted DWI in active areas |
| Cortical dysplasia | Congenital malformation; transmantle sign on MRI; blurring of grey-white junction; no mass effect |
| Ganglioglioma | Calcification more common, often presents with long-standing epilepsy |
| DNET (Dysembryoplastic neuroepithelial tumour) | Cortical location, often associated with drug-resistant epilepsy |
-
Fangusaro et al. Response assessment in paediatric low-grade glioma: recommendations from the Response Assessment in Pediatric Neuro-Oncology (RAPNO) working group. 2020. The Lancet. Oncology - Open in new tab. ↩