Glioblastoma¶
Summary
- Glioblastoma (GBM) is an aggressive primary brain tumour arising from glial cells
- Characterised by rapid growth, necrosis, and angiogenesis
- Presents with neurological symptoms and has poor prognosis despite multimodal treatment1
Pathophysiology¶
- Under WHO 2021, glioblastoma is by definition IDH-wildtype (IDH-mutant grade 4 tumours are now classified as astrocytoma)
- Molecular criteria can define GBM even without necrosis/microvascular proliferation: TERT promoter mutation, EGFR amplification, or +7/−10 chromosome copy-number change
- Highly invasive with marked angiogenesis and necrosis
Demographics¶
- Most common primary malignant brain tumour in adults
- Incidence: 3.2 per 100,000 person-years
- Median age at diagnosis: 64 years
- Male to female ratio: 1.6:1
- Risk factors:
- Ionizing radiation exposure
- Rare genetic syndromes (e.g., Li-Fraumeni syndrome, neurofibromatosis type 1)
Diagnosis¶
- Clinical presentation:
- Headaches
- Seizures
- Focal neurological deficits
- Cognitive changes
- Histopathology:
- WHO grade 4 astrocytoma
- Microvascular proliferation
- Pseudopalisading necrosis
- High mitotic activity
- Molecular markers:
- MGMT promoter methylation status
- IDH mutation status
- 1p/19q codeletion (to rule out oligodendroglioma)
Imaging¶
- MRI (preferred modality):
- T1-weighted with contrast: Ring-enhancing mass with central necrosis
- T2-weighted/FLAIR: Extensive peritumoural oedema
- DWI: Restricted diffusion in cellular components
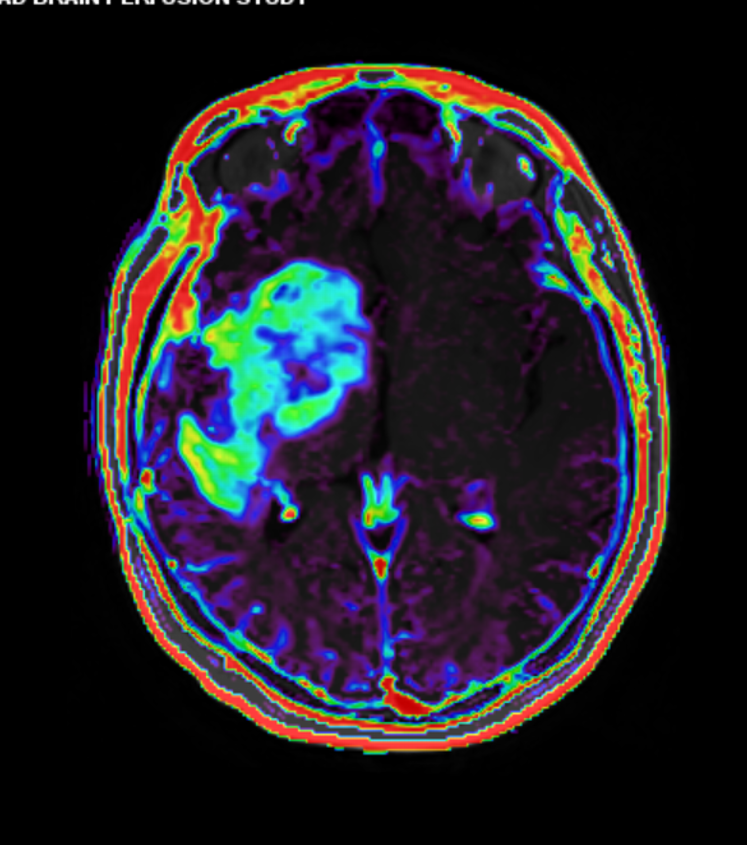
- Perfusion imaging: Increased relative cerebral blood volume
- CT:
- Hypodense mass with irregular enhancement
- Surrounding oedema and mass effect
- Advanced imaging techniques:
- MR spectroscopy: Elevated choline, reduced NAA, presence of lipid/lactate peak
- PET: Increased FDG uptake in high-grade components
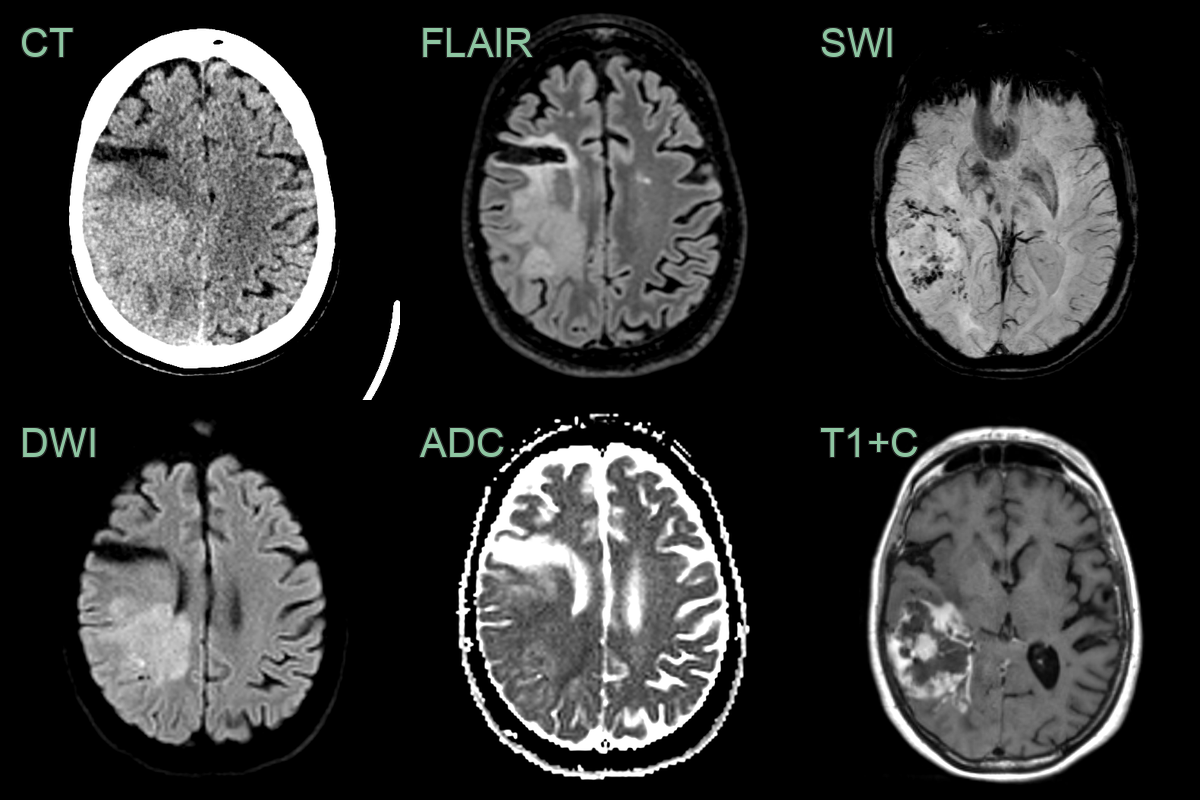
- 60-year-old patient, with a previous right MCA territory ischaemic stroke, presented with a left-sided homonymous hemianopia.
- CT showed a hyperdense mass lesion posterior to the old infarct.
- MRI showed a diffusion-restricting, peripherally enhancing mass lesion. SWI showed neovascularisation and microhaemorrhages within the lesion.
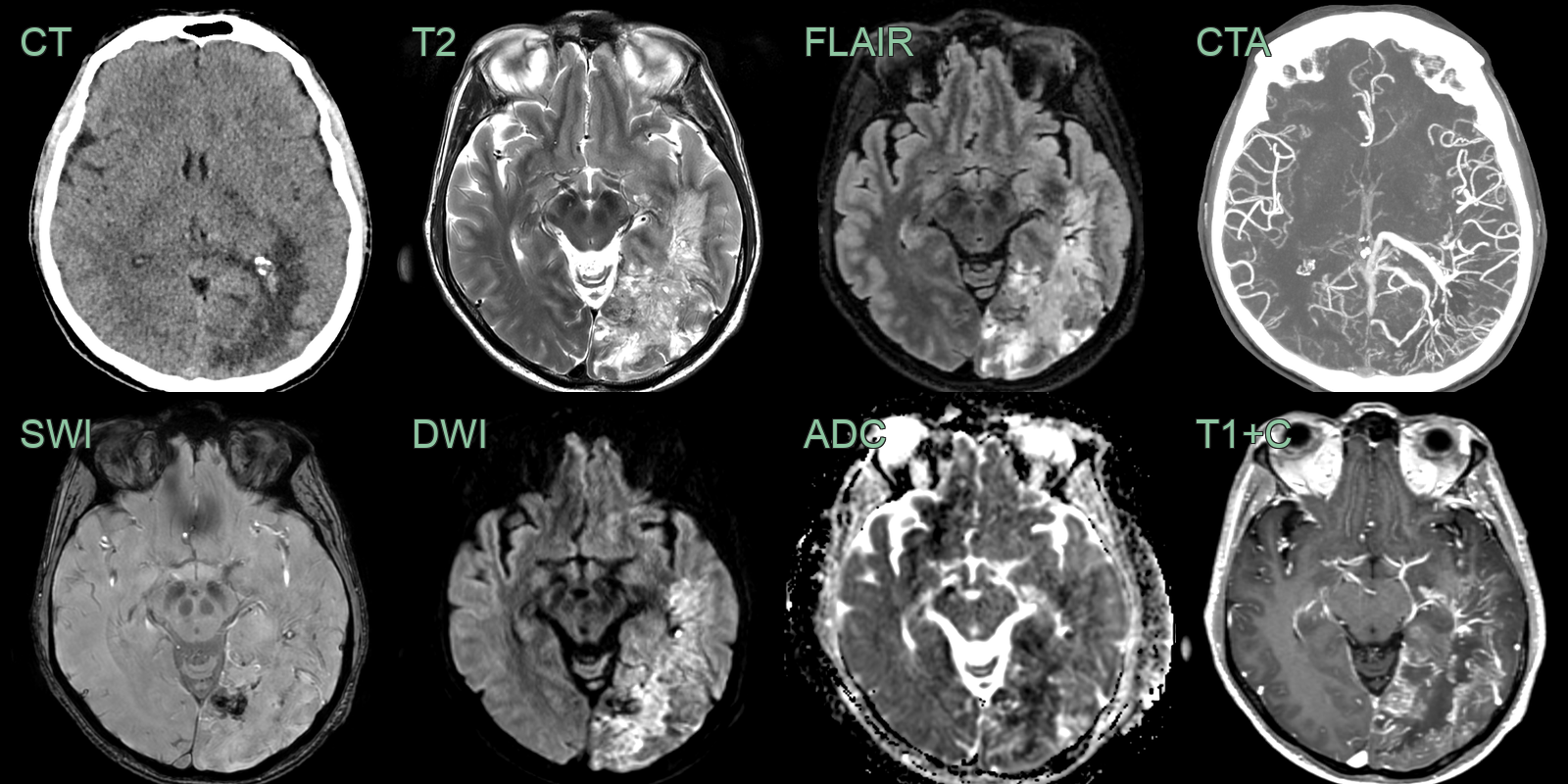
- A patient presented with a headache and on examination had a large right visual field defect.
- CT showed a larger left occipital lesion with striking (neo)vascularity.
- MRI showed a peripherally enhancing lesion causing diffusion restriction and containing small regions of blood product.
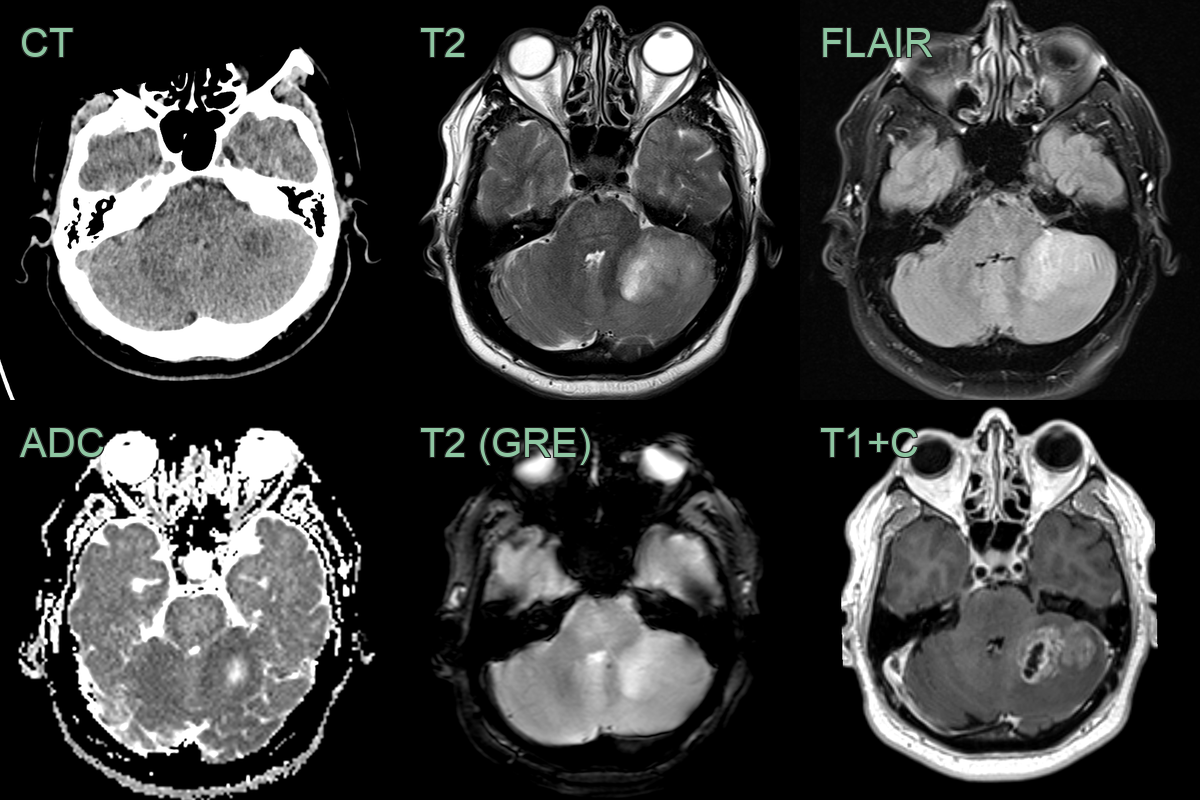
- 65-year-old patient presented with headache, nausea, vomiting and speech disturbance.
- Imaging showed a peripherally enhancing, centrally necrotic, left cerebellar mass lesion.
- ADC values were lower in the periphery of the tumour indicating hypercellularity.
- Unusually for the cerebellum, histopathology revealed a glioblastoma.
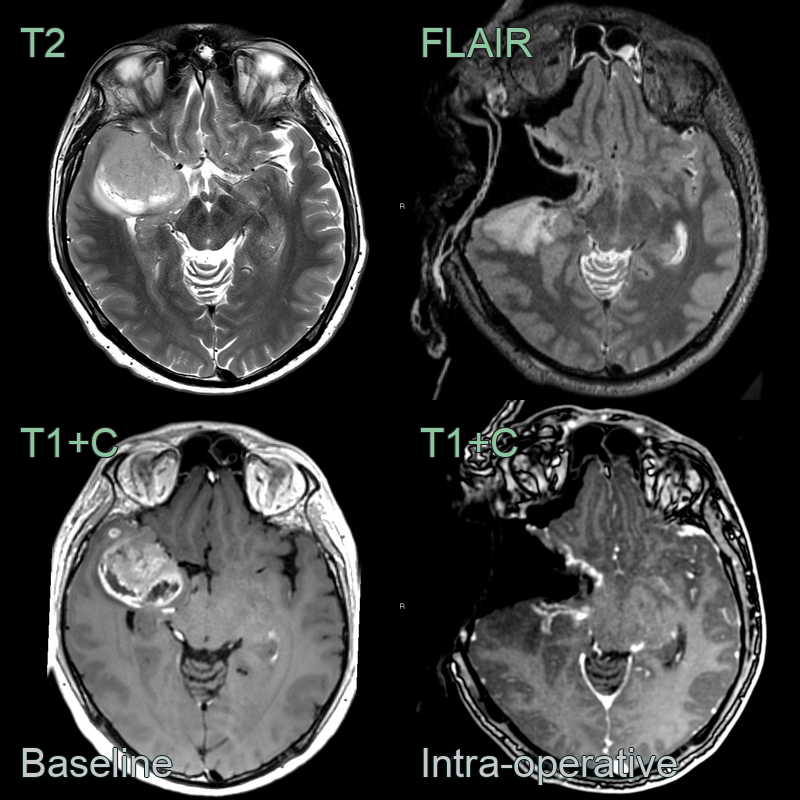
- A 50-year-old patient presented following a seizure.
- MRI showed a large right temporal peripherally enhancing lesion with areas of diffusion restriction (not shown).
- Intra-operative MRI was used to guide a maximal safe resection.
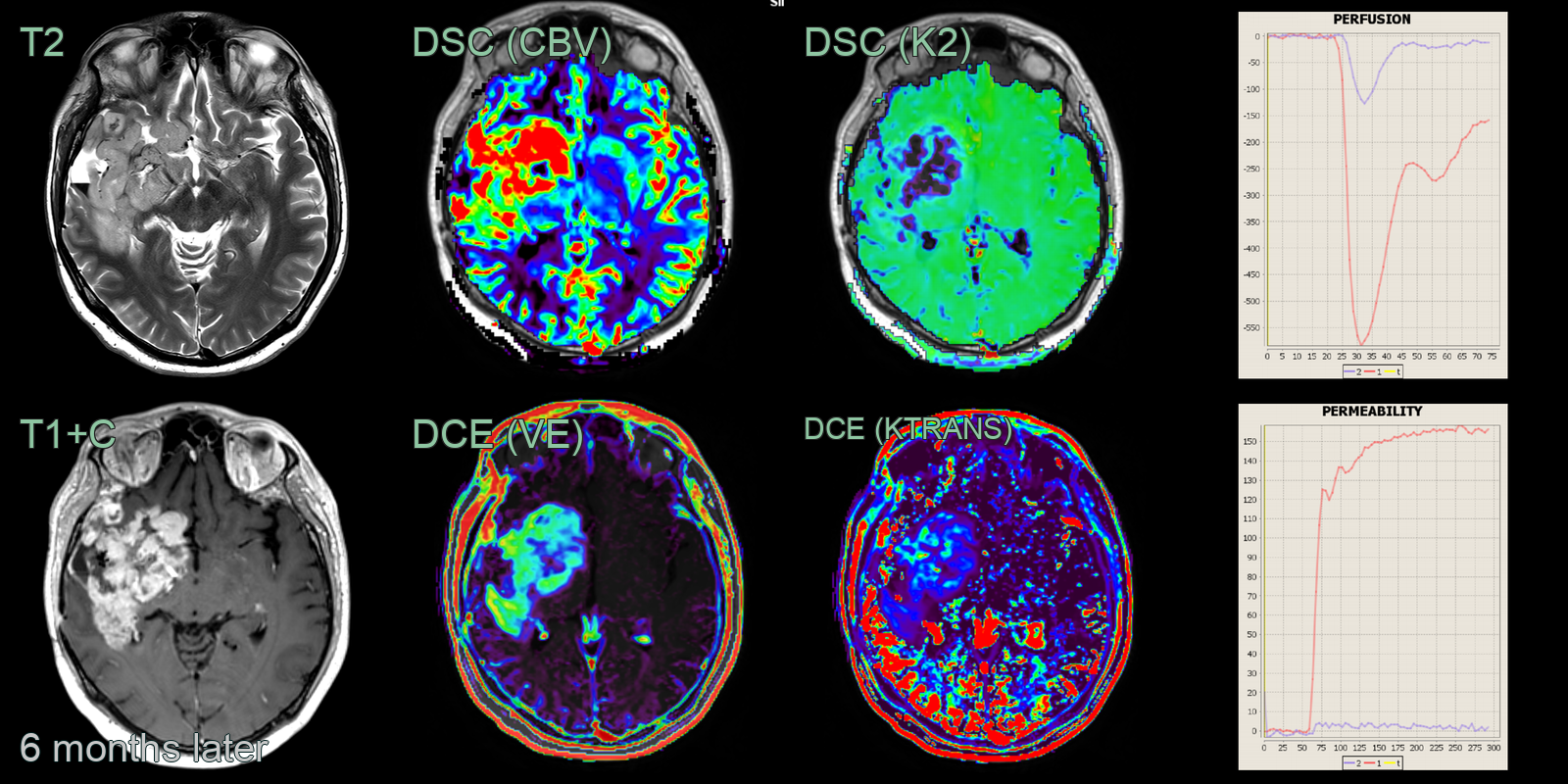
- Within 6 months, there was a large volume of disease progression. While obvious on structural imaging, this was confirmed on DSC perfusion (elevated CBV and abnormal K2) and DCE perfusion (elevated Ktrans and VE and a Type 2 curve).
Treatment¶
- Maximal safe resection with concurrent/adjuvant temozolomide and radiotherapy (Stupp protocol); prognosis remains poor
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Metastatic brain tumour | Multiple lesions at grey-white junction; surrounding vasogenic oedema disproportionate to lesion size; no corpus callosum crossing |
| Primary CNS lymphoma | Homogeneous enhancement without central necrosis; restricted diffusion on DWI; hyperdense on non-contrast CT; periventricular location |
| Brain abscess | Thin smooth ring enhancement; restricted DWI centrally; no irregular thickened wall; may have satellite lesions |
| Anaplastic astrocytoma | Less necrosis; less enhancement or no enhancement; less vasogenic oedema |
| Oligodendroglioma | Calcifications on CT; cortical-based; "chicken wire" vascular pattern; less necrosis |
| Meningioma | Extra-axial location, dural tail sign |
| Demyelinating disease | Incomplete ring enhancement, periventricular location |
| Radiation necrosis | History of radiation therapy, more well-defined borders |
| Subacute stroke | Follows vascular territory, diffusion restriction in acute phase |
| Tumefactive multiple sclerosis | Incomplete ring enhancement, less mass effect |
-
Lim et al. Current state of immunotherapy for glioblastoma. 2018. Nature reviews. Clinical oncology - Open in new tab. ↩