Cerebral Autosomal Dominant Arteriopathy with Subcortical Infarcts and Leukoencephalopathy (CADASIL)¶
Summary
- CADASIL is a hereditary small vessel disease characterised by recurrent subcortical infarcts, cognitive decline, and migraine with aura
- Caused by mutations in the NOTCH3 gene, leading to accumulation of granular osmiophilic material (GOM) in small arteries
- MRI shows characteristic white matter hyperintensities, lacunar infarcts, and microbleeds, particularly in the anterior temporal lobes and external capsule1
Pathophysiology¶
- Autosomal dominant inheritance pattern
- Mutations in NOTCH3 gene on chromosome 19p13.1
- Encodes a transmembrane receptor protein involved in cell signaling
- Accumulation of GOM in vascular smooth muscle cells
- Leads to thickening of vessel walls and luminal narrowing
- Progressive degeneration of vascular smooth muscle cells
- Impaired cerebral blood flow and chronic ischaemia
Demographics¶
- Prevalence: 2-5 per 100,000 individuals
- Age of onset: typically 30-50 years
- No gender predilection
- Most common in Caucasian populations, but reported worldwide
Diagnosis¶
- Clinical presentation:
- Recurrent ischaemic strokes
- Cognitive decline and dementia
- Migraine with aura
- Mood disturbances
- Genetic testing:
- Sequencing of NOTCH3 gene
- Skin biopsy:
- Electron microscopy to detect GOM in arterioles
Imaging¶
- MRI findings:
- T2/FLAIR hyperintensities in white matter
- Anterior temporal lobe involvement (90% of cases)
- External capsule involvement (80% of cases)
- Lacunar infarcts in basal ganglia, thalamus, and pons
- Microbleeds on susceptibility-weighted imaging (SWI)
- Cerebral atrophy in advanced stages
- CT findings:
- Less sensitive than MRI
- May show hypodensities in white matter and lacunar infarcts
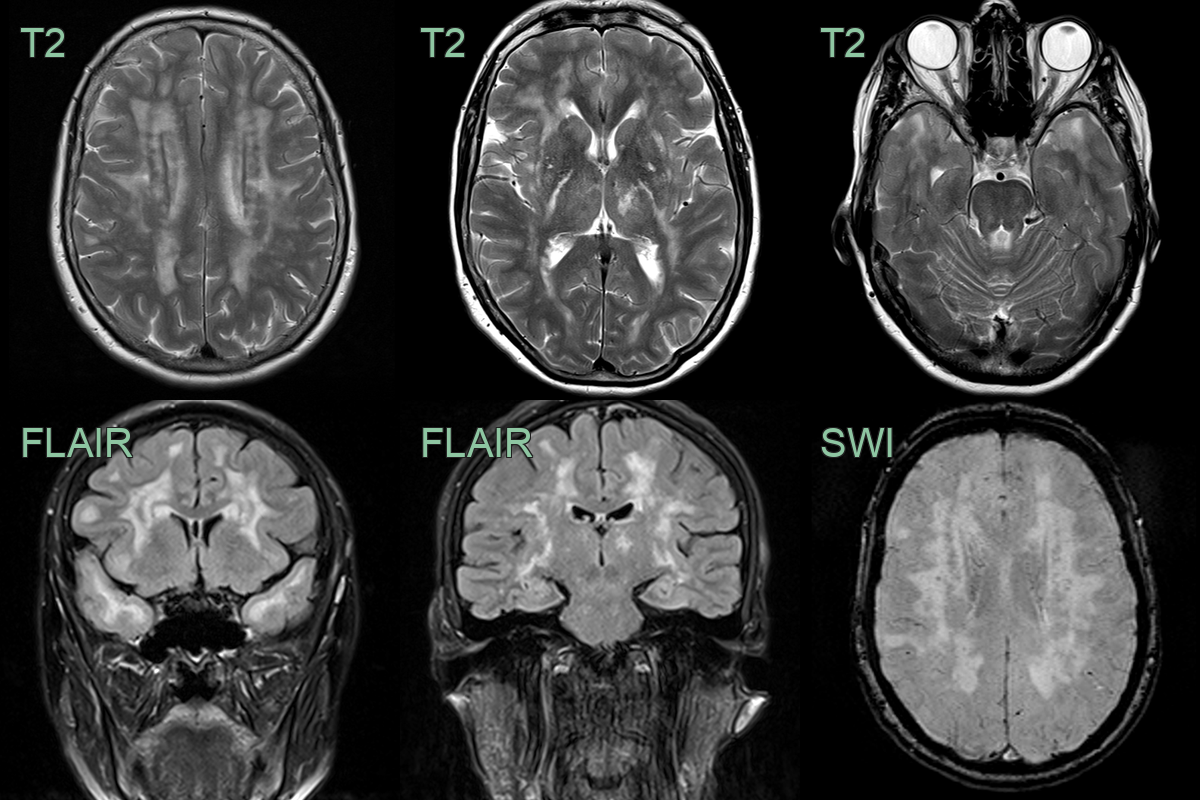
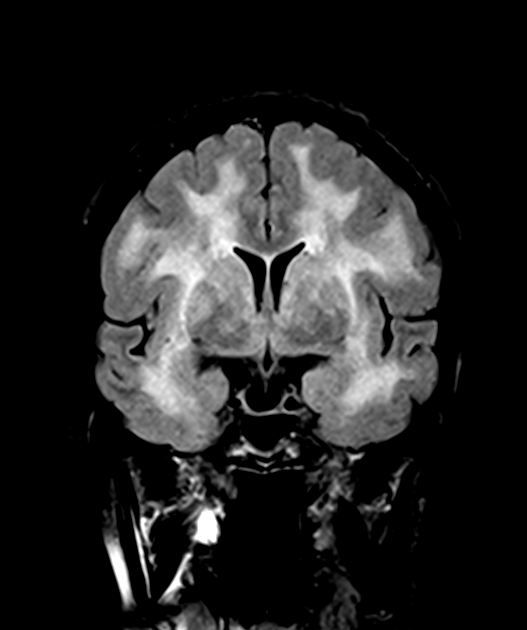
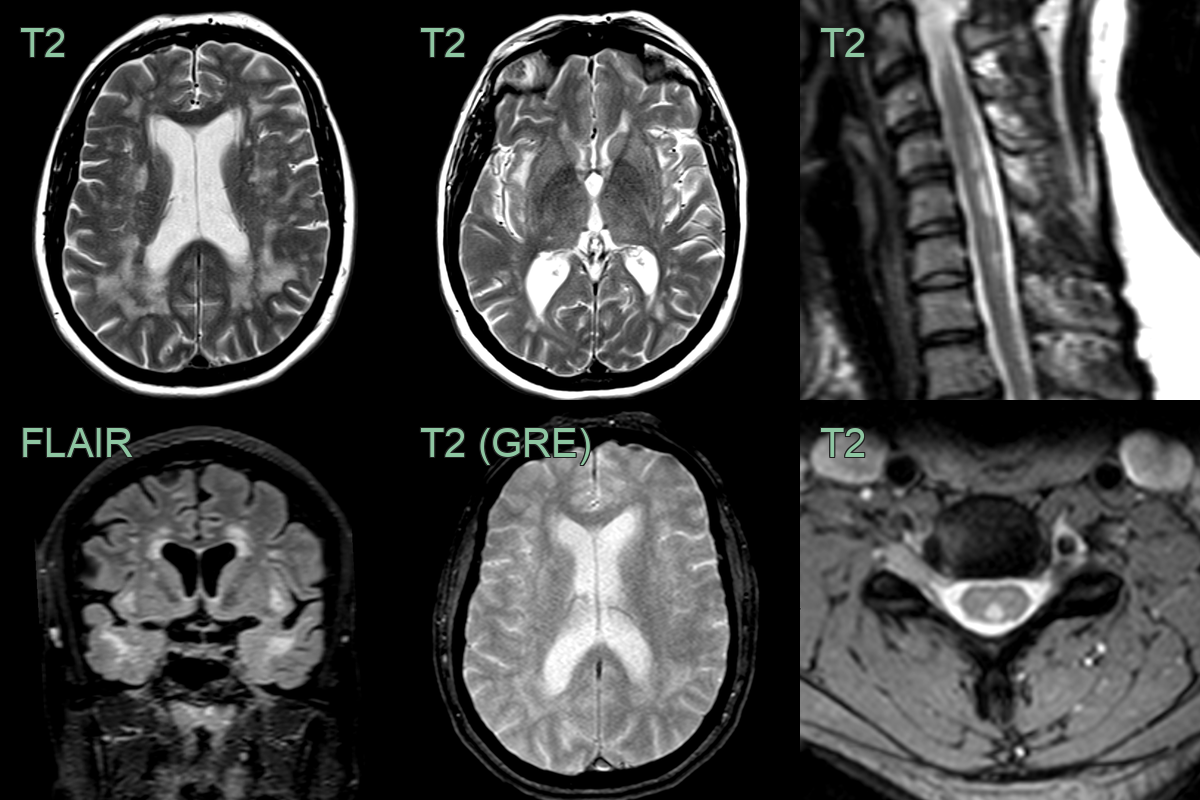
- A 55-year-old patient with no cardiovascular risk factors presented with recurrent headache.
- MRI showed a confluent leukoencephalopathy, involving the external capsules and anterior temporal lobes, and lacunar infarcts.
- There were deep and lobar microhaemorrhages.
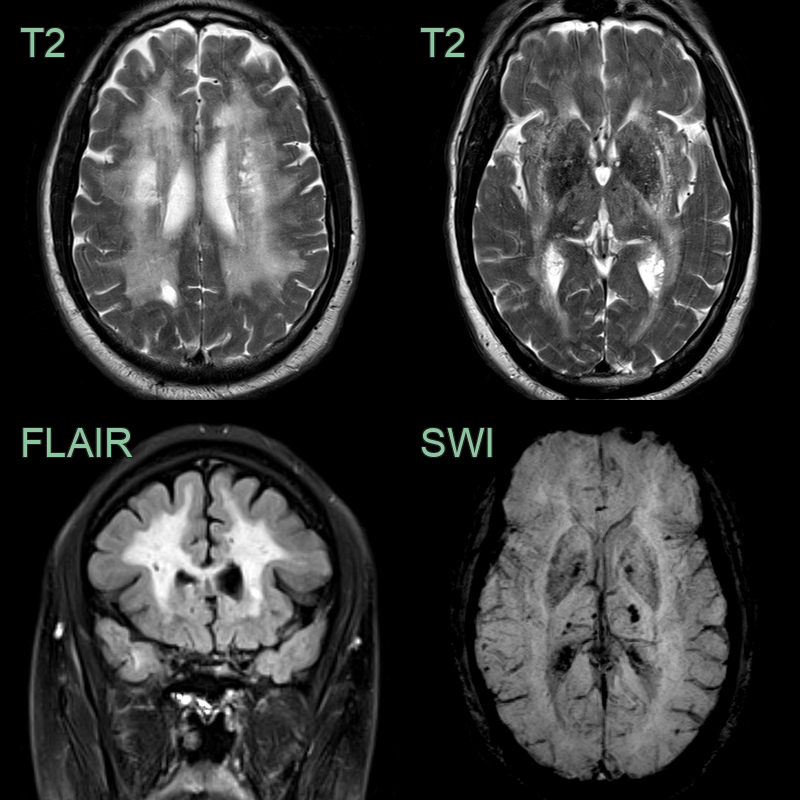
- 50-year-old patient with no cardiovascular risk factors had recurrent strokes.
- MRI showed a severe burden of small vessel disease, multiple lacunar infarcts and mixed distribution microhaemorrhages.
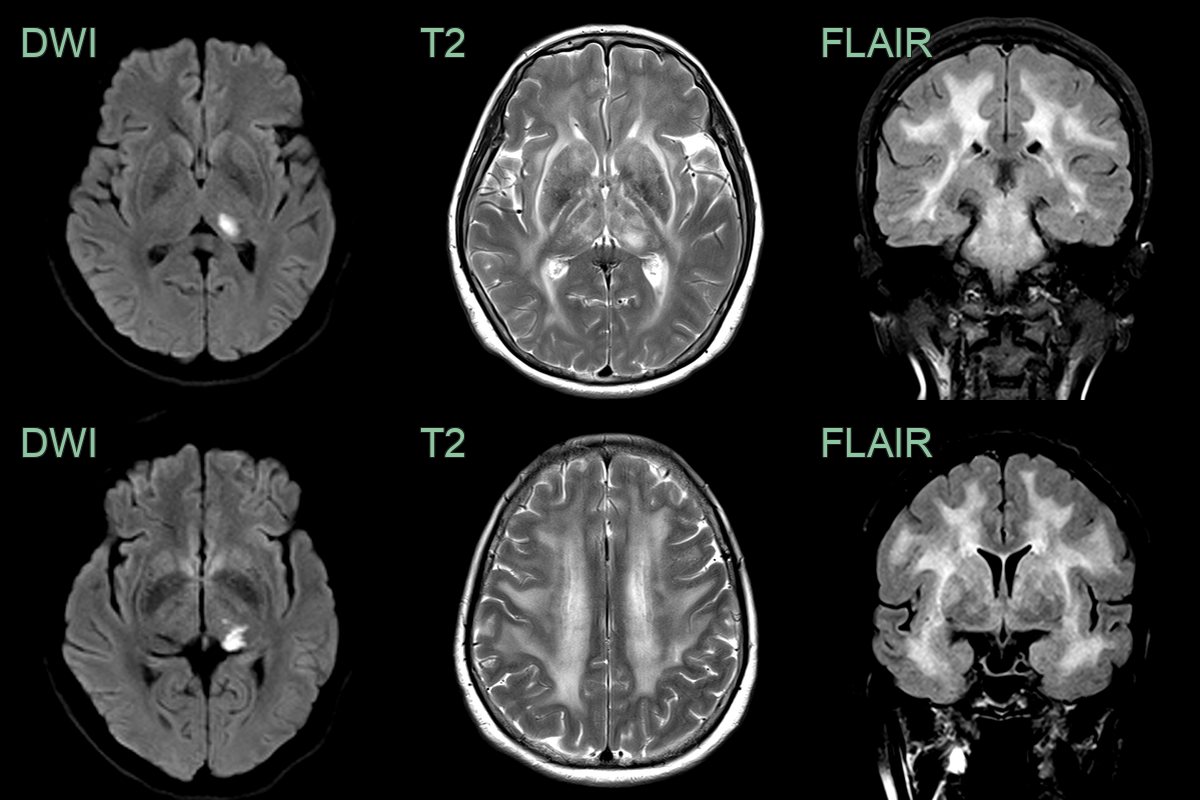
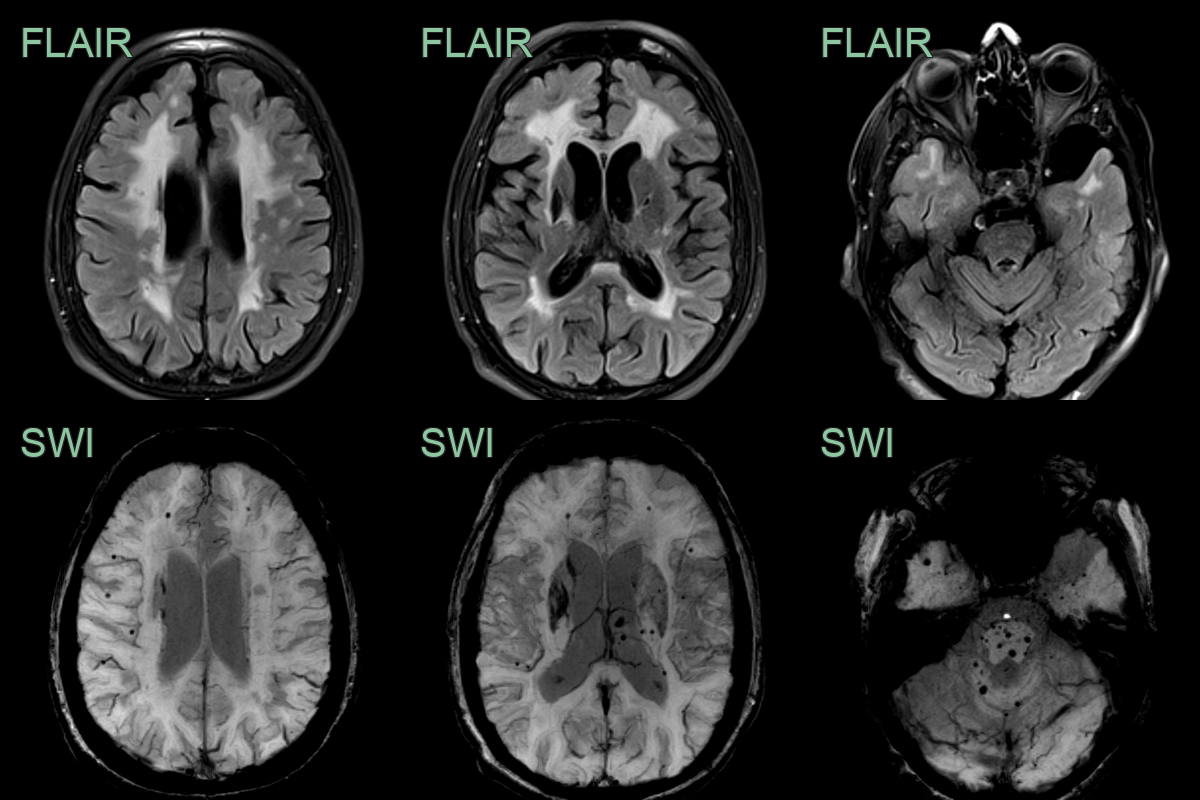
- 50-year-old patient presented with a homonymous hemianopia and mixed sensory and motor deficits.
- MRI showed an acute left thalamic infarct and a diffuse leukoencephalopathy that involved the external capsules and anterior temporal lobes.
- Alongside the classical intracranial features of CADASIL, MRI showed multiple dorsal column hyperintensities.
- With no evidence of a metabolic or demyelinating cause, findings were ascribed to a CADASIL-related myelopathy.
Treatment¶
- No cure; antiplatelet therapy, vascular risk-factor control and migraine management
Differential diagnosis¶
| Imaging differential | Differentiating feature |
|---|---|
| Sporadic small vessel disease / Binswanger | Confluent deep white matter disease that characteristically spares the anterior temporal poles and external capsule |
| Cerebral amyloid angiopathy | Lobar, posterior-predominant microbleeds and cortical superficial siderosis; temporal poles spared |
| Fabry disease | Pulvinar T1 hyperintensity; posterior white matter change |
| CARASIL / CARASAL and other hereditary SVD | Overlapping white matter disease; distinguished genetically |
| MELAS | Cortical/subcortical lesions not confined to vascular territories, with a lactate peak on MRS |
-
Ruchoux et al. CADASIL: Cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy. 1997. Journal of neuropathology and experimental neurology - Open in new tab. ↩