Cerebral Amyloid Angiopathy (CAA)¶
Summary
- Cerebral amyloid angiopathy is characterised by amyloid-β deposition in cerebral blood vessels
- Typically presents with lobar haemorrhages in older adults
- Imaging findings include microbleeds, cortical superficial siderosis, and white matter hyperintensities
Pathophysiology¶
- Accumulation of amyloid-β protein in walls of cortical and leptomeningeal vessels
- Leads to vessel wall weakening and increased risk of haemorrhage
- Associated with Alzheimer's disease but can occur independently
- Genetic factors (e.g., APOE ε4 allele) increase susceptibility
Demographics¶
- Primarily affects older adults (>55 years)
- Prevalence increases with age
- No significant gender predilection
- More common in individuals of European and Asian descent
Diagnosis¶
- Clinical presentation:
- Lobar intracerebral haemorrhage
- Transient focal neurological episodes
- Cognitive decline
- Diagnosis uses the Boston criteria v2.0, which add non-haemorrhagic markers (severe centrum semiovale perivascular spaces and multispot white matter hyperintensities) to the haemorrhagic features1
Imaging¶
- CT findings:
- Lobar haemorrhages, often multiple and recurrent
- Subarachnoid haemorrhage
- MRI findings:
- Gradient-echo (GRE) or susceptibility-weighted imaging (SWI):
- Microbleeds in cortical/subcortical regions
- Cortical superficial siderosis
- T2-weighted and FLAIR:
- White matter hyperintensities
- Enlarged perivascular spaces in centrum semiovale
- PET imaging:
- Amyloid PET can detect vascular amyloid deposition
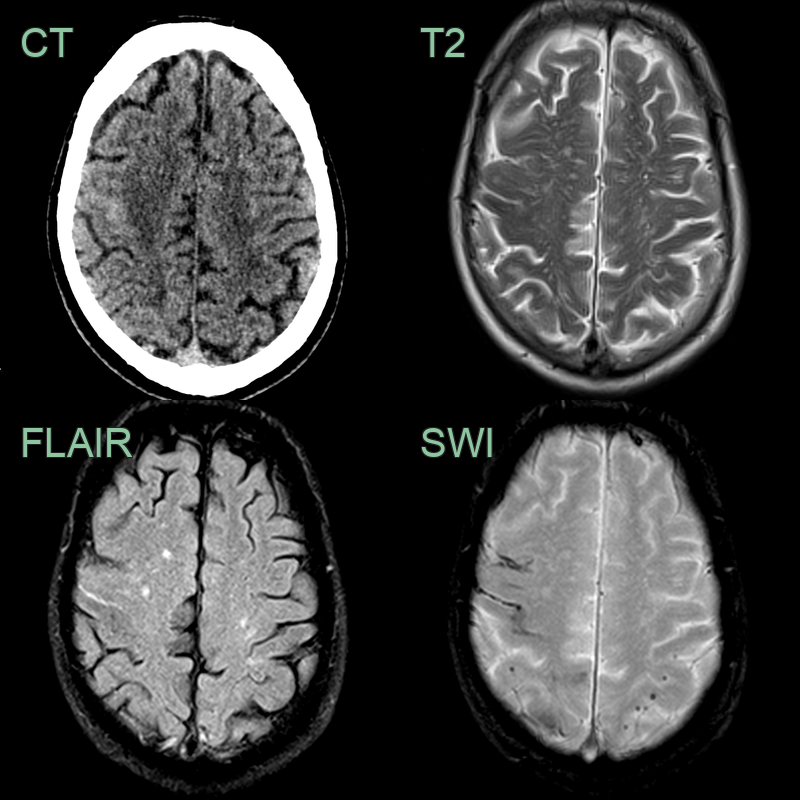
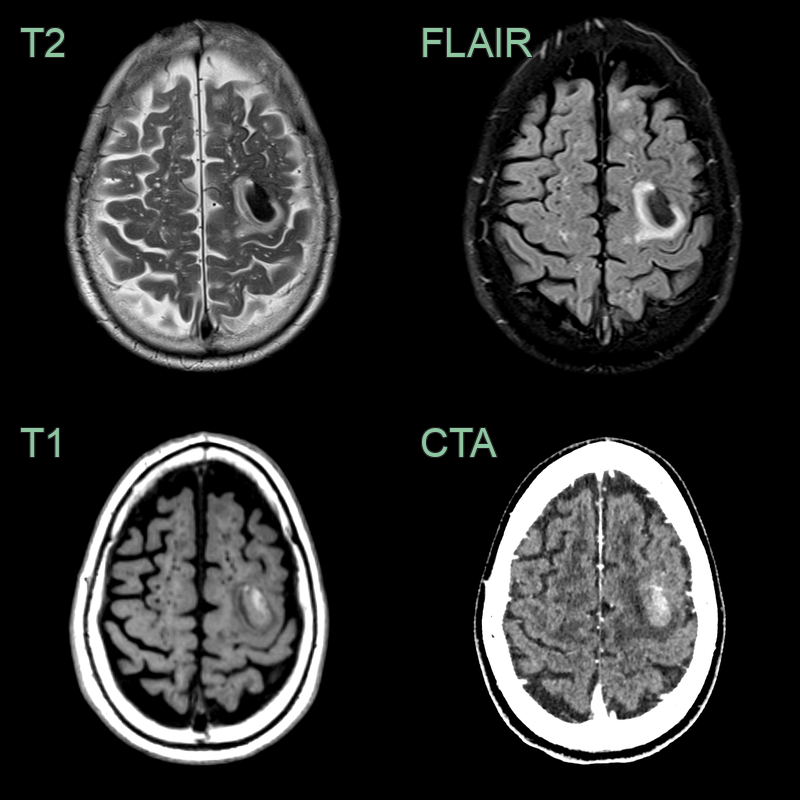
- 75-year-old patient presented with abnormal sensation in the left arm.
- CT showed blood product in the right pre-central gyrus.
- On MRI, there was sulcal hyperintensity on FLAIR consistent with recent blood product.
- Enlarged perivascular spaces, multi-spot small vessel disease, superficial siderosis and lobar microhaemorrhages indicated a diagnosis of TFNEs secondary to CAA.
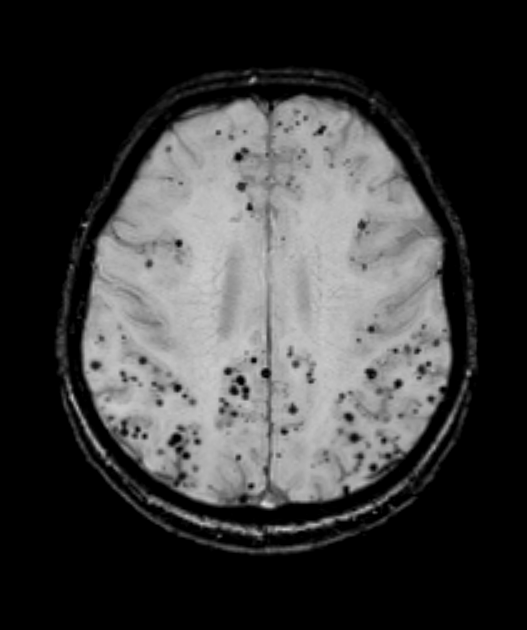
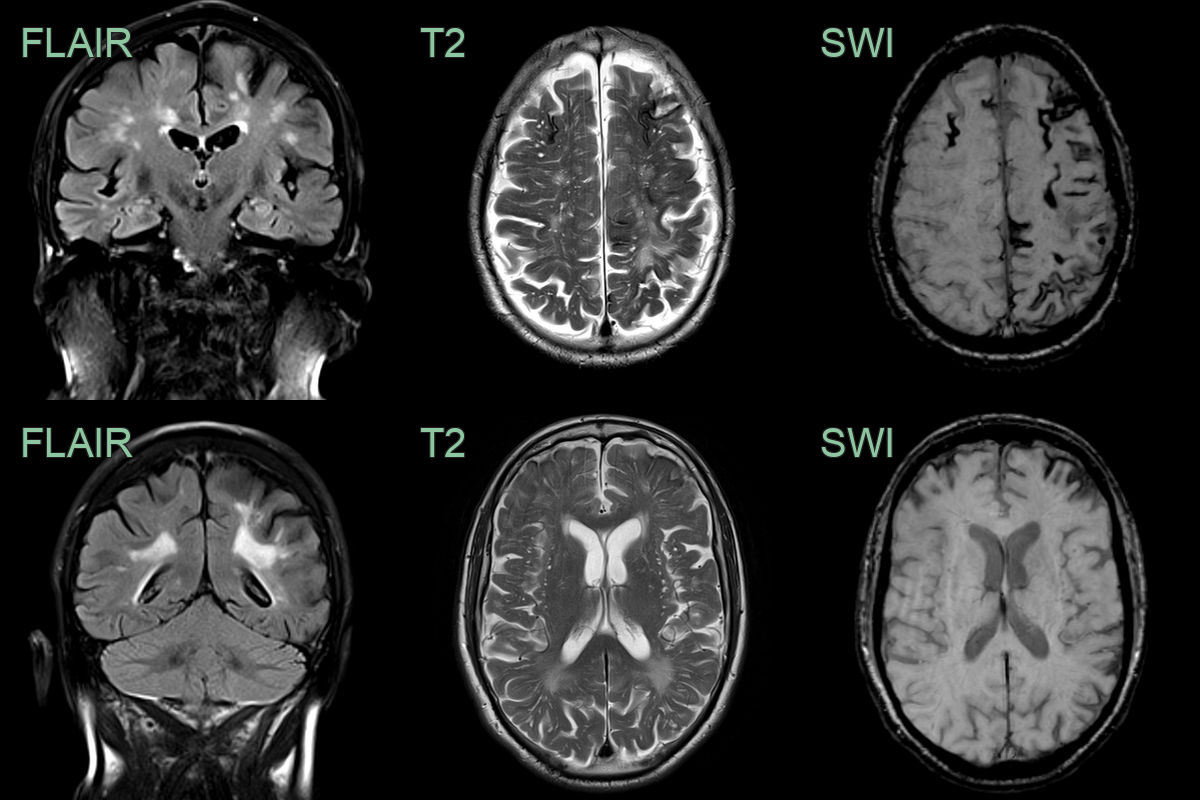
- Multi-spot small vessel disease predominantly in the centrum semiovale, enlarged perivascular spaces and innumerable peripheral microhaemorrhages.
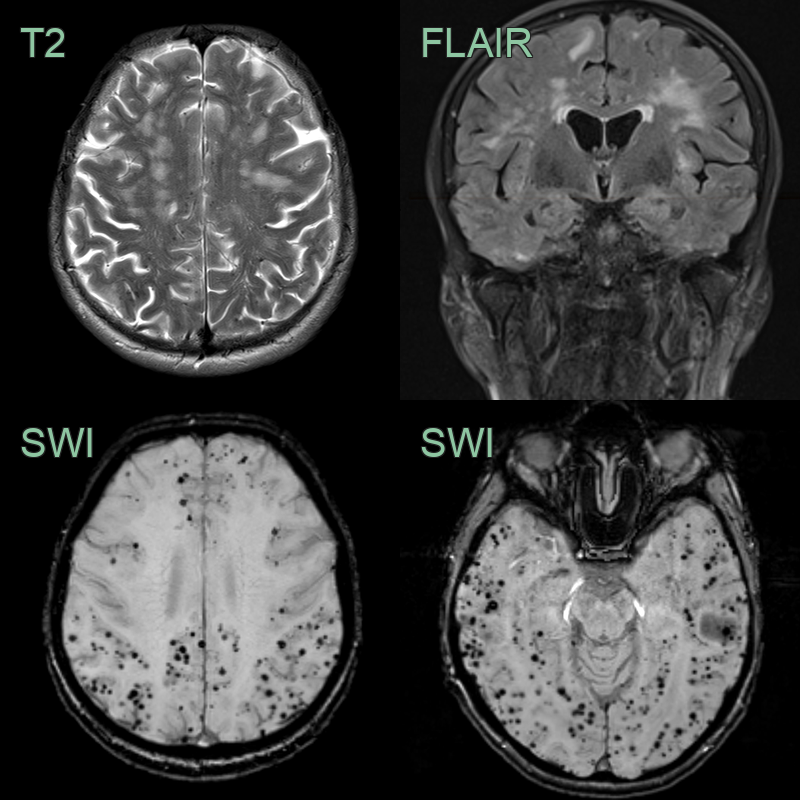
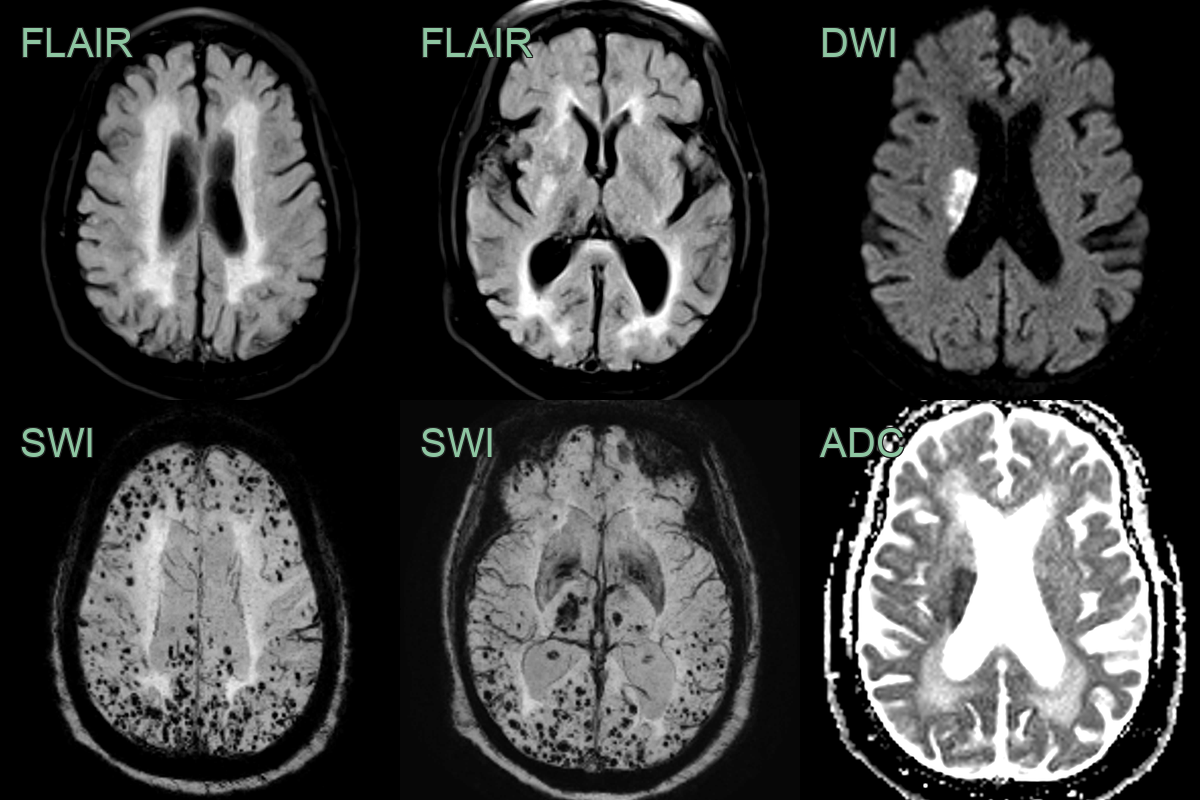
- Multi-spot small vessel disease, enlarged perivascular spaces, lobar microhaemorrhages, and extensive superficial siderosis indicate cerebral amyloid angiopathy.
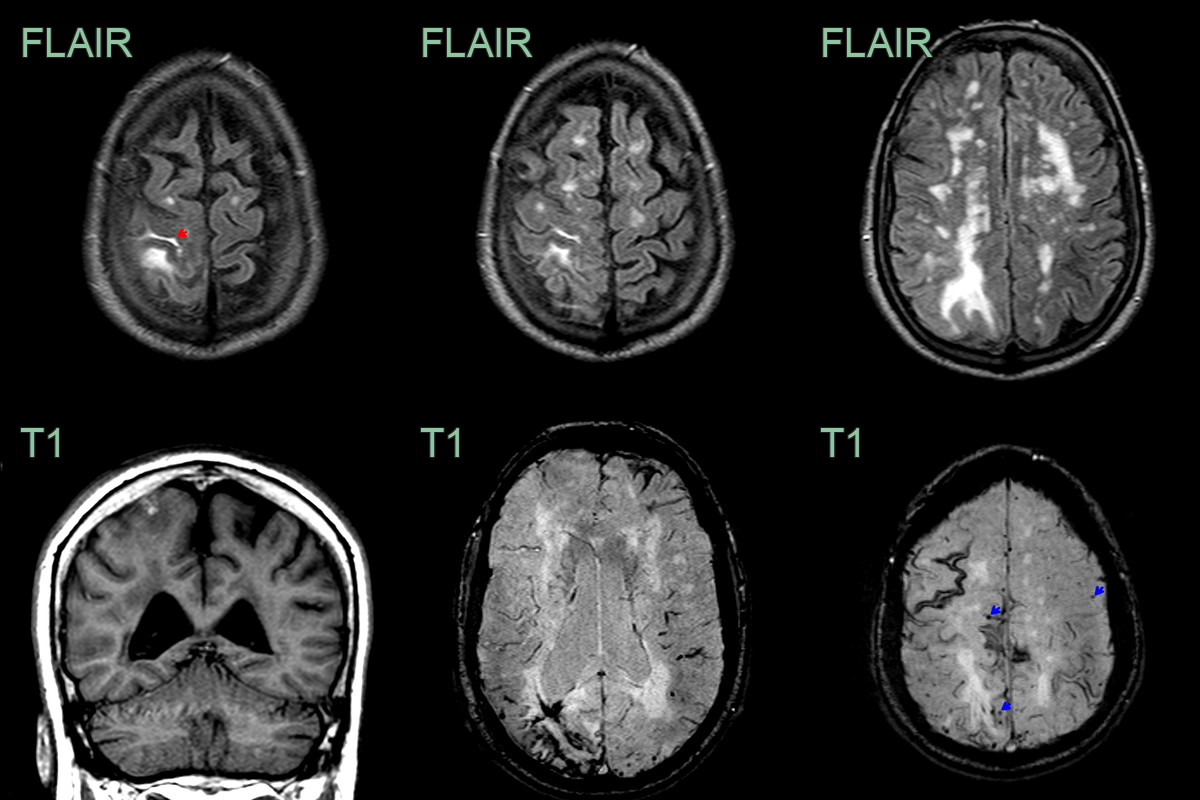
- There was sulcal FLAIR hyperintensity in the right superior frontal sulcus and the left calcarine sulcus (not shown) that were associated with the left sided motor and right visual field TFNEs.
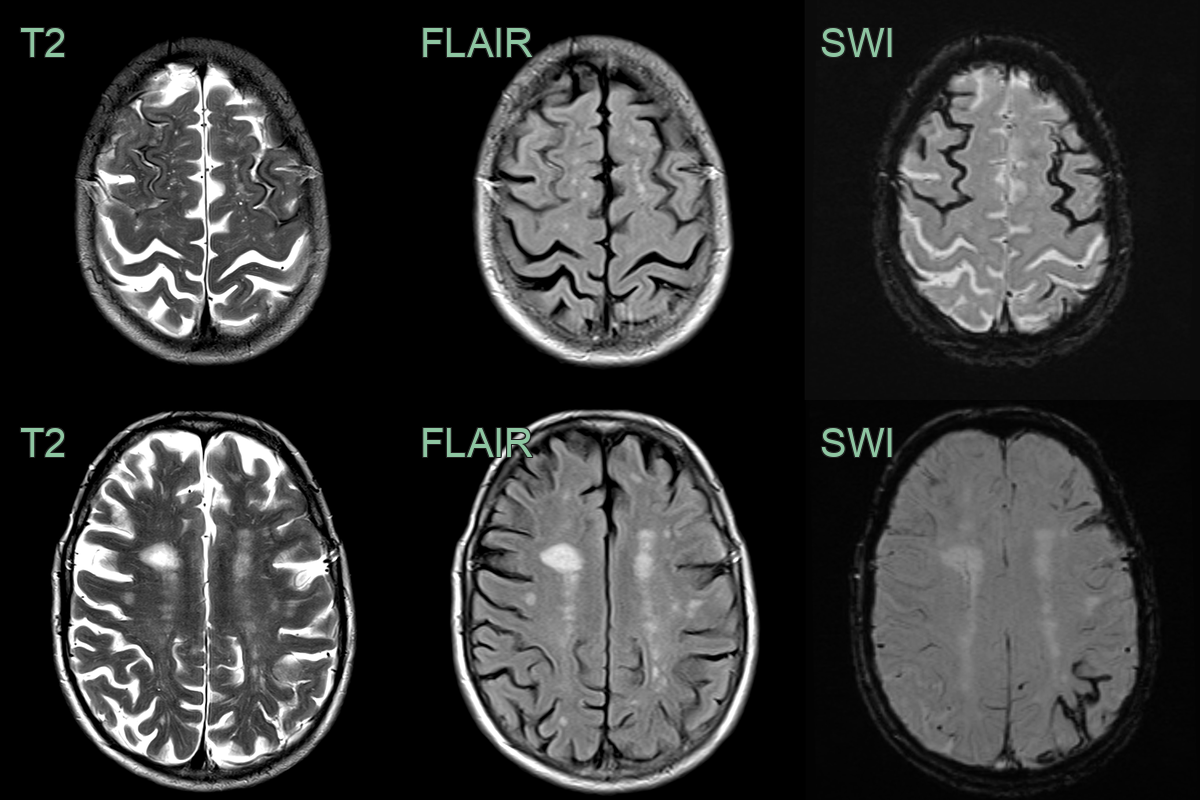
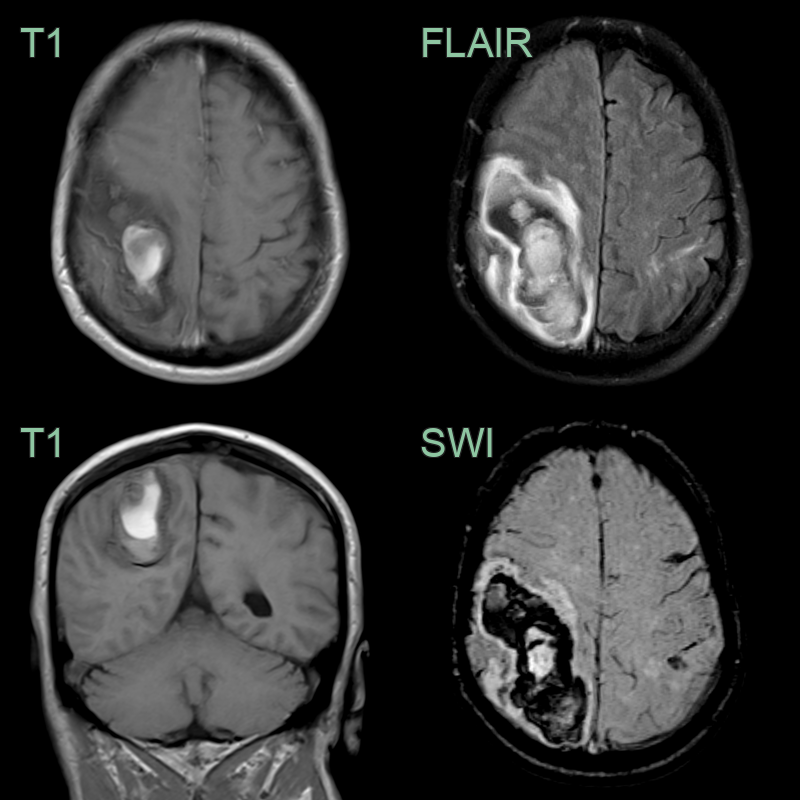
- 75-year-old patient presented with right arm weakness.
- The initial MRI showed a lobar haemorrhage affecting the left precentral gyrus. There was a multi-spot pattern of (posterior-predominant) small vessel disease, many enlarged subcortical perivascular spaces, and extensive superficial siderosis but only a few lobar microhaemorrhages.
- A 75-year-old patient presented with left sided weakness.
- MRI showed an acute infarct in the right corona radiata.
- SWI showed florid microhaemorrhages in a mixed distribution - both deep (likely representing hypertensive arteriolosclerosis) and lobar (likely representing cerebral amyloid angiopathy).
- A 65-year-old patient presented with headache and left sided weakness.
- MRI showed a large lobar haematoma in the right parietal lobe.
- There was a trace of acute blood in the left post-central gyrus (based on FLAIR hyperintensity).
- While there were no white matter features of CAA, the combination of the superficial siderosis over the left frontal lobe and the lobar haematoma were sufficient to meet criteria for probable CAA.
- A 70-year-old patient presented with transient sensory disturbance in the left arm and left side of the face.
- MRI showed subarachnoid blood/effusion in the right central sulcus (red arrows) as a cause of the TFNE.
- SWI showed cortical microhaemorrhages (green arrows) and many areas of superficial siderosis.
Treatment¶
- No specific therapy; blood-pressure control and cautious avoidance of antithrombotics
- Note that amyloid-targeting immunotherapy for Alzheimer's can precipitate ARIA in patients with CAA
Differential diagnosis (multiple microbleeds / lobar haemorrhage)¶
| Imaging differential | Differentiating feature |
|---|---|
| Hypertensive microangiopathy | Microbleeds in deep structures (basal ganglia, thalamus, pons) rather than a lobar/cortical distribution |
| Diffuse axonal injury | Microbleeds at the grey–white junction, corpus callosum and brainstem; trauma history |
| Radiation-induced microbleeds/cavernomas | Confined to the prior radiation field |
| Multiple cavernomas (familial) | Popcorn lesions with complete haemosiderin rims; some larger with internal architecture |
| CADASIL | Anterior temporal and external capsule white matter change with deep microbleeds |
-
Charidimou et al. The Boston criteria version 2.0 for cerebral amyloid angiopathy: a multicentre, retrospective, MRI–neuropathology diagnostic accuracy study. 2022. The Lancet Neurology - Open in new tab. ↩