Hypertensive Microangiopathy¶
Summary
- Chronic hypertension-induced damage to small blood vessels in the brain
- Characterised by arteriolar wall thickening, luminal narrowing, and white matter changes
- Imaging findings include white matter hyperintensities, lacunar infarcts, and microbleeds1
Pathophysiology¶
- Sustained hypertension leads to:
- Arteriolar wall thickening and remodelling
- Endothelial dysfunction and blood-brain barrier disruption
- Impaired cerebral autoregulation
- Consequences include:
- Chronic hypoperfusion of deep white matter
- Ischaemic damage to small penetrating arteries
- Increased risk of lacunar infarcts and microbleeds
Demographics¶
- Prevalence increases with age and duration of hypertension
- More common in:
- Elderly population (>65 years)
- Individuals with poorly controlled hypertension
- Patients with diabetes mellitus or chronic kidney disease
Diagnosis¶
- Clinical presentation:
- Often asymptomatic in early stages
- Cognitive decline, gait disturbances, and mood changes in advanced cases
- Neurological examination may reveal:
- Subtle cognitive deficits
- Mild parkinsonian features
- Pseudobulbar palsy in severe cases
- Neuropsychological testing can detect early cognitive impairment
Imaging¶
- MRI is the modality of choice:
- T2-weighted and FLAIR sequences:
- Periventricular and deep white matter hyperintensities
- Lacunar infarcts in basal ganglia, thalamus, and pons
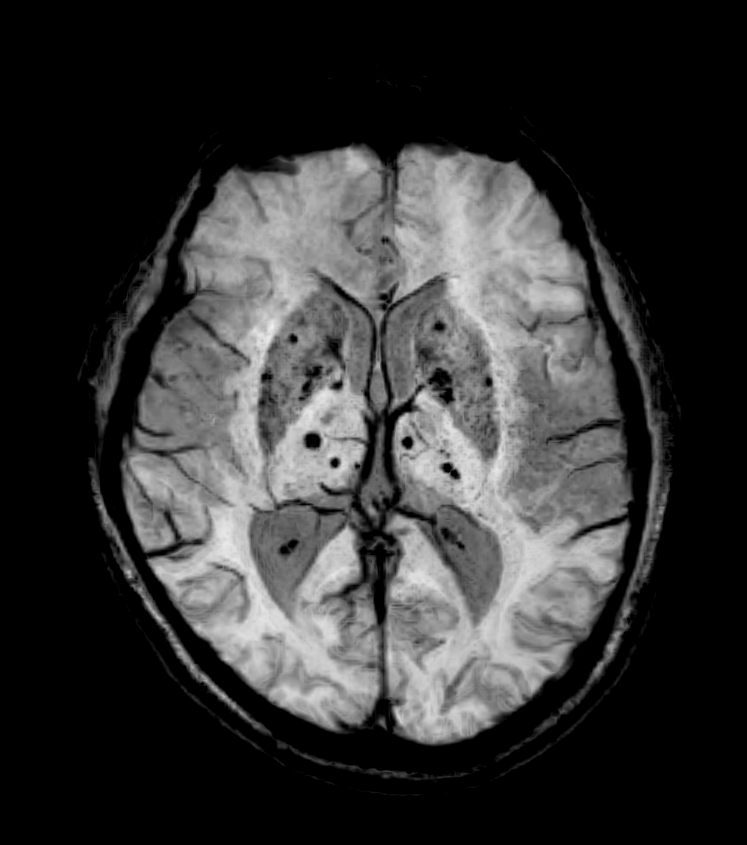
- Gradient-echo or susceptibility-weighted imaging:
- Microbleeds, typically in basal ganglia and thalamus
- Diffusion tensor imaging:
- Reduced fractional anisotropy in affected white matter
- CT may show:
- Hypodense areas in white matter
- Lacunar infarcts
- Limited sensitivity for microbleeds
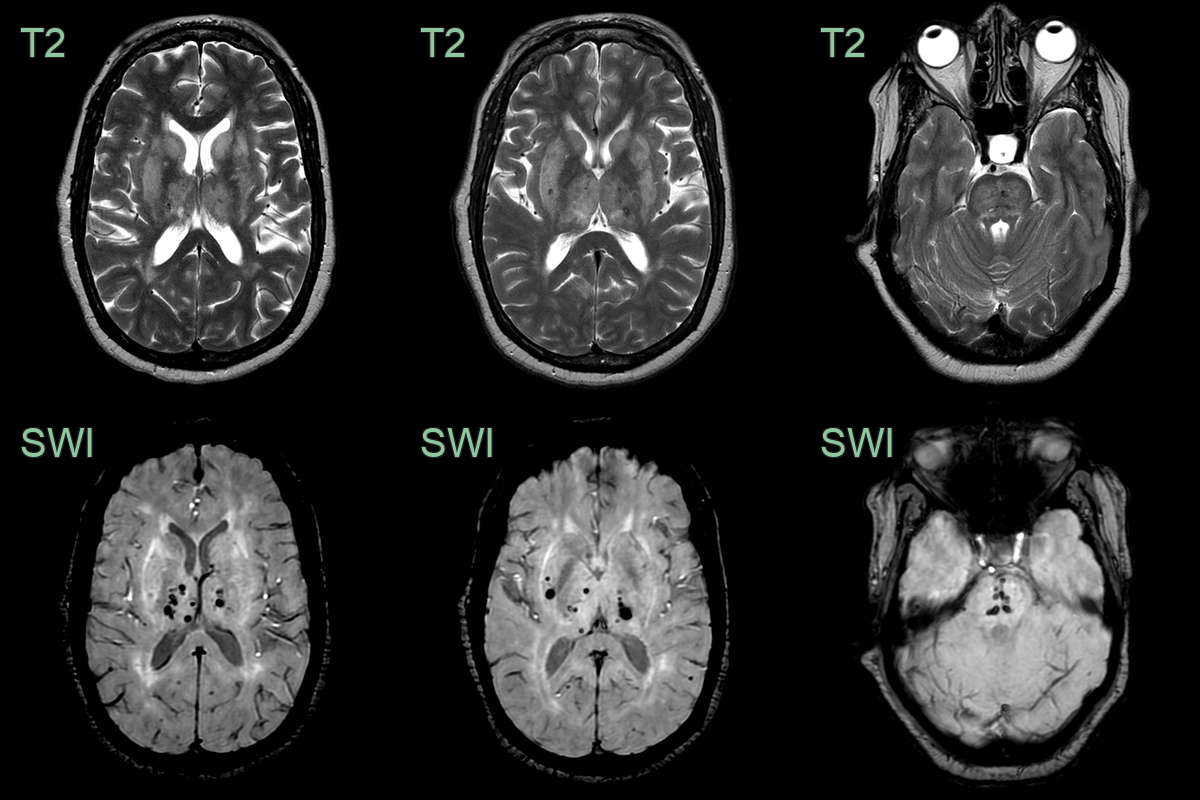
- A 60-year-old patient with chronic kidney disease and poorly controlled hypertension presented after a TIA.
- MRI showed hyperintensity of the deep grey nuclei and deep subcortical white matter, consistent with severe small vessel disease.
- The pattern of microhaemorrhages, exclusively involving the deep white matter and pons, are consistent with hypertensive microangiopathy.
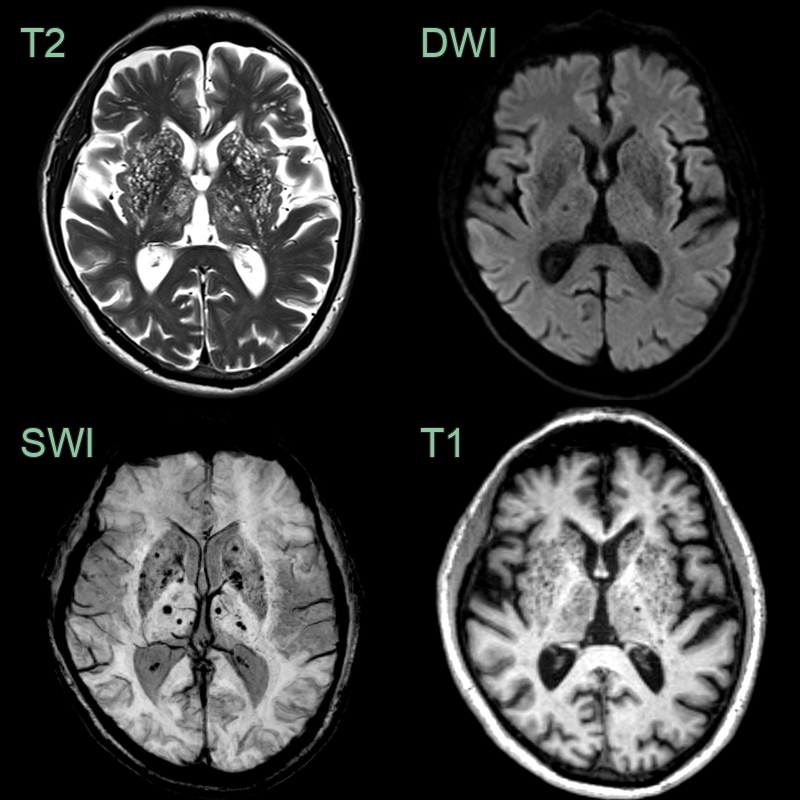
- A 50-year-old patient with poorly controlled hypertension had an MRI for headache.
- T2-weighted imaging showed striking widening of the perivascular spaces in deep grey nuclei representing état criblé.
- SWI showed exclusively deep microhaemorrhages.
Treatment¶
- Blood-pressure control. The deep (basal ganglia, thalamus, pons) distribution of microbleeds distinguishes it from the lobar pattern of amyloid angiopathy
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Cerebral Amyloid Angiopathy | Lobar and cortical-subcortical microbleeds on GRE/SWI; posterior predominance; superficial siderosis |
| Multiple Sclerosis | Ovoid periventricular lesions; calloso-septal interface ("Dawson's fingers"); no deep microbleeds |
| Cerebral Autosomal Dominant Arteriopathy with Subcortical Infarcts and Leukoencephalopathy (CADASIL) | Anterior temporal pole and external capsule FLAIR hyperintensity; subcortical lacunar infarcts; microbleeds |
| Vasculitis | Beaded appearance of vessels on angiography; vessel wall enhancement on high-resolution MRI; multifocal cortical and subcortical infarcts |
-
Wardlaw et al. Small vessel disease: mechanisms and clinical implications. 2019. The Lancet. Neurology - Open in new tab. ↩