Cauda Equina Compression¶
Summary
- Compression of nerve roots below L1-L2 spinal level
- Caused by space-occupying lesions in the spinal canal
- Presents with lower back pain, saddle anesthesia, and bladder/bowel dysfunction1
Pathophysiology¶
- Compression of lumbosacral nerve roots within the spinal canal
- Common causes:
- Herniated lumbar disc (most frequent)
- Spinal stenosis
- Tumour (primary or metastatic)
- Trauma
- Epidural abscess or haematoma
- Leads to ischaemia and potential permanent nerve damage if not treated promptly
Demographics¶
- Incidence: 1-3 cases per 100,000 population per year
- Most common in adults aged 30-50 years
- Slightly more prevalent in males
- Risk factors:
- Degenerative disc disease
- History of spinal surgery
- Spinal trauma
- Coagulopathies (for epidural haematoma)
Diagnosis¶
- Clinical presentation:
- Low back pain
- Bilateral sciatica
- Saddle anesthesia
- Bladder and/or bowel dysfunction
- Lower extremity weakness
- Physical examination:
- Reduced perianal sensation
- Decreased anal sphincter tone
- Lower extremity motor and sensory deficits
- Diagnostic criteria:
- One or more of: bladder/bowel dysfunction, reduced sensation in saddle area, sexual dysfunction
- Plus one or more of: low back pain, bilateral sciatica, lower extremity sensorimotor deficits
Imaging¶
- MRI:
- Gold standard for diagnosis
- T1-weighted: assess vertebral body alignment and marrow changes
- T2-weighted: evaluate disc herniations, spinal cord, and nerve root compression
- Gadolinium-enhanced: useful for detecting tumours or infections
- CT myelography:
- Alternative when MRI is contraindicated
- Shows compression of nerve roots and thecal sac
- Plain radiographs:
- Limited utility, may show vertebral body misalignment or fractures
- CT:
- Useful for assessing bony abnormalities and fractures
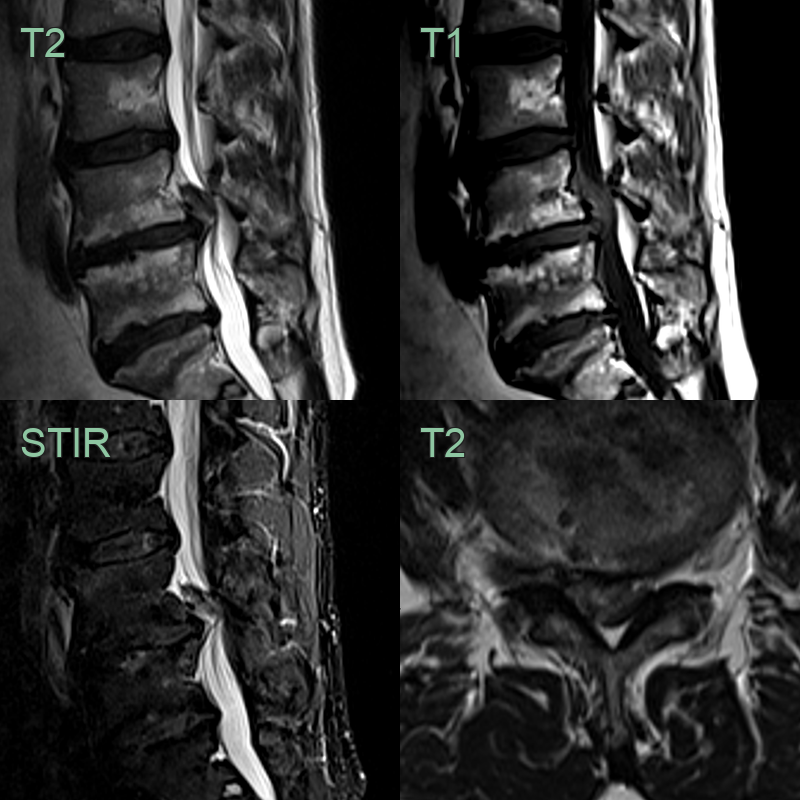
- 50-year-old patient presented with acute onset severe sciatica.
- At L4-5, a cranially migrated disc extrusion caused effacement of all CSF and compression of the cauda equina.
Treatment¶
- Urgent surgical decompression, ideally early, for progressive deficit
- Directed at the cause (discectomy, tumour resection, abscess/haematoma evacuation)
Differential diagnosis (compressive/enhancing cauda equina)¶
| Imaging differential | Differentiating feature |
|---|---|
| Central disc extrusion | Disc-signal material effacing the thecal sac, contiguous with the parent disc |
| Epidural abscess | Rim-enhancing epidural collection, often with adjacent discitis and endplate erosion |
| Epidural haematoma | Non-enhancing epidural collection with blood-product signal; anticoagulation/procedure history |
| Epidural metastasis / lymphoma | Enhancing marrow-replacing or epidural soft tissue with cord/root compression |
| Drop metastases / leptomeningeal disease | Nodular enhancing deposits coating the roots rather than a single compressive mass |
| Guillain-Barré / CIDP | Smooth thickening and enhancement of the roots without a compressive lesion |
-
B Rydevik. Neurophysiology of cauda equina compression. 1993. Acta orthopaedica Scandinavica. Supplementum - Open in new tab. ↩