Cerebral Malaria¶
Summary
- Severe complication of Plasmodium falciparum infection affecting the central nervous system
- Characterised by impaired consciousness, seizures, and coma
- Diagnosis based on clinical presentation, blood smears, and neuroimaging findings1
Pathophysiology¶
- Caused by sequestration of parasitised erythrocytes in cerebral microvasculature
- Leads to:
- Microvascular obstruction
- Endothelial activation
- Blood-brain barrier disruption
- Cerebral oedema
- Inflammatory response contributes to neurological damage
- Potential long-term cognitive and neurological sequelae
Demographics¶
- Most common in children under 5 years in sub-Saharan Africa
- Also affects adults in regions with lower malaria transmission
- Travellers from non-endemic areas at risk when visiting malaria-endemic regions
- Mortality rate ranges from 15-25% despite treatment
Diagnosis¶
- Clinical criteria:
- Unarousable coma (Glasgow Coma Scale ≤9)
- Exclusion of other causes of encephalopathy
- Laboratory findings:
- Positive blood smear for P. falciparum
- Rapid diagnostic tests for malaria antigens
- Lumbar puncture to rule out other causes of coma
- Neuroimaging to assess complications and exclude differential diagnoses
Imaging¶
- CT findings:
- Brain swelling (50-75% of cases)
- Focal hypodensities suggesting infarction
- Rarely, haemorrhage
- MRI findings:
- More sensitive than CT for detecting subtle abnormalities
- T2 and FLAIR hyperintensities in:
- Cortical grey matter
- Basal ganglia
- Corpus callosum
- Brainstem
- Diffusion-weighted imaging may show cytotoxic oedema
- Susceptibility-weighted imaging can detect microhaemorrhages
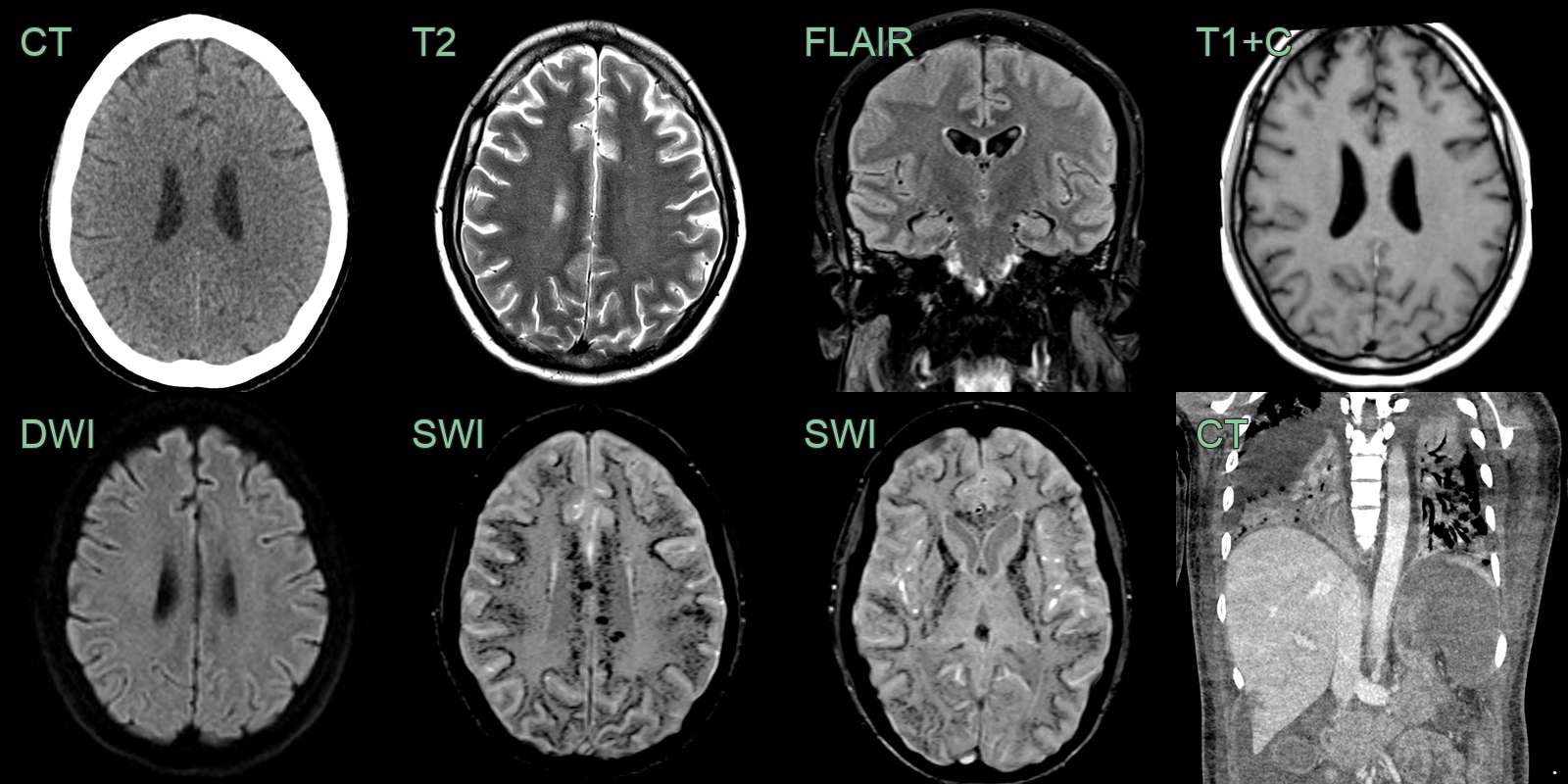
- A 40-year-old patient became obtunded 1 month after return from a region endemic for malaria.
- MRI showed the brain parenchyma appearing normal on T2 and FLAIR and DWI - there was no oedema or ischaemic changes.
- However, SWI showed extensive juxtacortical and deep white matter foci of susceptibility artefact (representing microhaemorrhages and/or microthrombi).
- Chest imaging showed bilateral lung consolidation, splenomegaly (with infarction) and small regions of hepatic infarcts.
Treatment¶
- Prompt IV artesunate and supportive care; mortality remains high
Differential diagnosis¶
| Differential Diagnosis | Distinguishing Feature |
|---|---|
| Intracranial Haemorrhage | Focal neurological deficits; CT scan shows bleeding |
| Acute disseminated encephalomyelitis (ADEM) | Multifocal subcortical and deep white matter T2 hyperintensities, often with partial ring enhancement |
| Viral encephalitis (e.g. Japanese encephalitis) | Bilateral thalamic and basal ganglia T2 hyperintensity; mesial temporal involvement in HSV |
| Osmotic demyelination | Central pontine symmetric T2 hyperintensity sparing peripheral rim |
| Posterior reversible encephalopathy syndrome (PRES) | Parieto-occipital vasogenic oedema pattern, reversible on follow-up |
-
Luzolo et al. Cerebral malaria. 2019. Brain research bulletin - Open in new tab. ↩