Chagas Disease¶
Summary
- Chagas disease is a parasitic infection caused by Trypanosoma cruzi
- Transmitted primarily by triatomine bugs in endemic areas of Latin America
- Characterised by acute and chronic phases, with potential cardiac and gastrointestinal complications1
Pathophysiology¶
- Caused by the protozoan parasite Trypanosoma cruzi
- Transmission:
- Vector-borne: Triatomine bugs (kissing bugs)
- Non-vector: Blood transfusion, organ transplantation, congenital transmission
- Disease progression:
- Acute phase: High parasitaemia, mild symptoms
- Indeterminate phase: Asymptomatic, low parasitaemia
- Chronic phase: Organ damage (cardiac, gastrointestinal)
Demographics¶
- Endemic in 21 Latin American countries
- Estimated 6-7 million people infected worldwide
- Increasing prevalence in non-endemic areas due to migration
- Risk factors:
- Living in rural areas with poor housing conditions
- Poverty and lack of access to healthcare
Diagnosis¶
- Acute phase:
- Microscopic examination of blood smears
- PCR for T. cruzi DNA
- Chronic phase:
- Serological tests (ELISA, IFA, RIPA)
- At least two positive tests required for confirmation
- Diagnostic challenges:
- Low sensitivity in chronic phase due to low parasitaemia
- Cross-reactivity with other parasitic infections
Imaging¶
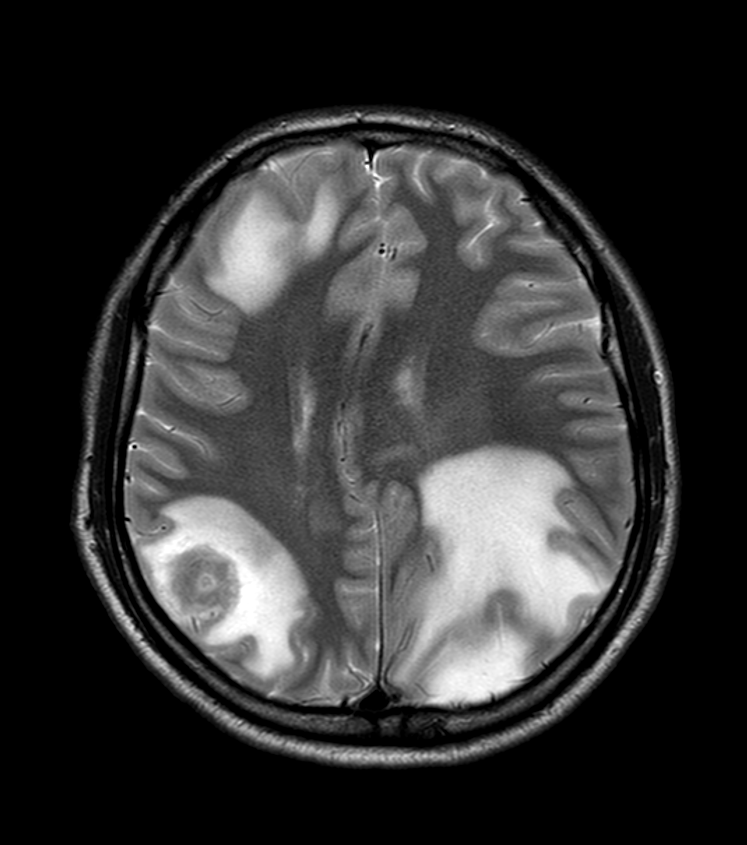
- CNS disease occurs chiefly as reactivation in immunocompromised patients (e.g. HIV), producing a necrotising encephalitis / "chagoma"
- MRI:
- One or several ring- or peripherally-enhancing lesions with surrounding vasogenic oedema, favouring the white matter and basal ganglia
- Variable haemorrhage; the principal differential is toxoplasmosis
- Systemically, Chagas causes a dilated cardiomyopathy and mega-oesophagus/megacolon
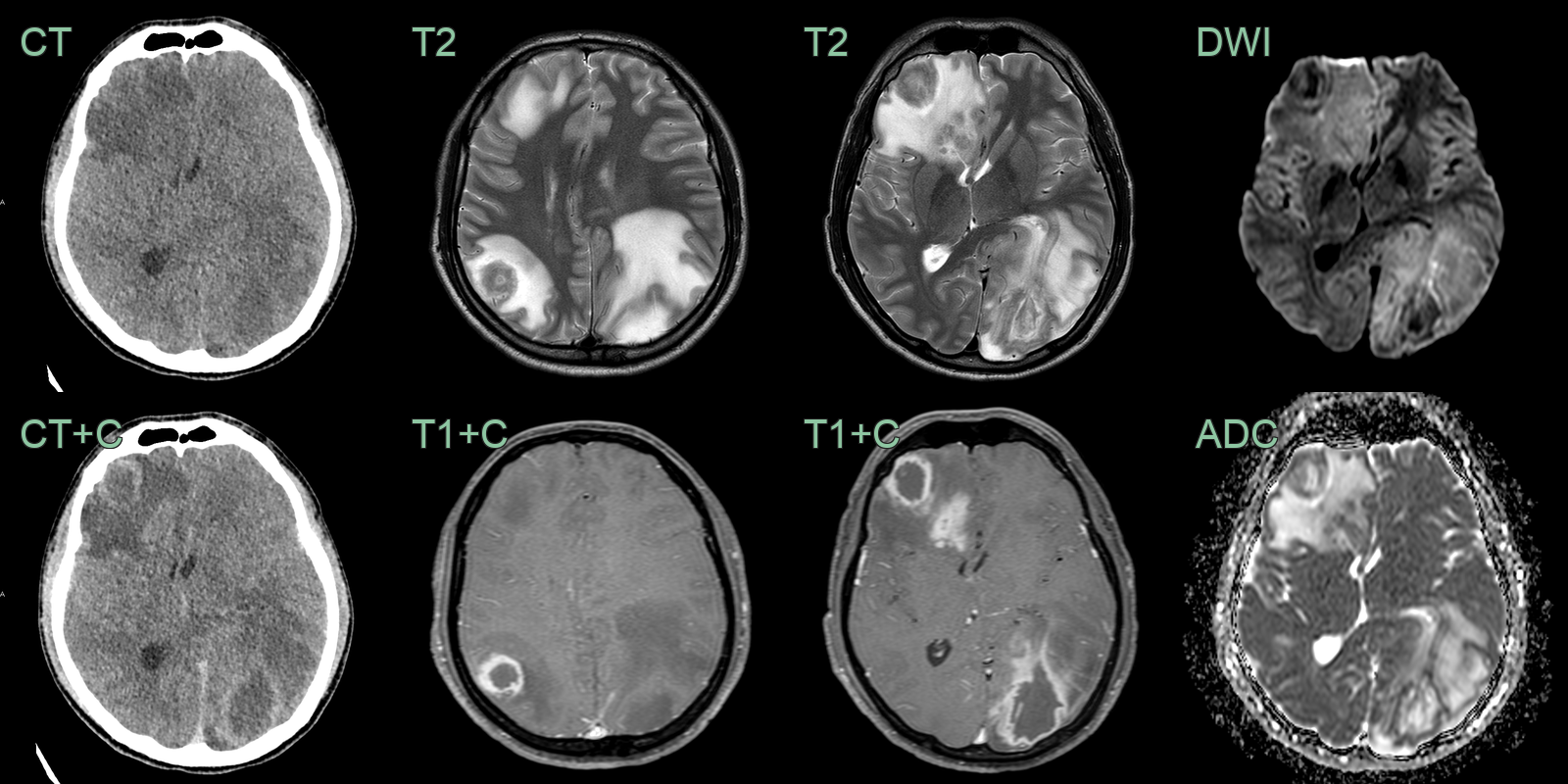
- A 25-year-old patient presented with reduced GCS and headache.
- CT and MRI showed multiple peripherally enhancing lesions with surrounding vasogenic oedema without diffusion restriction.
- A new diagnosis of HIV was made with a CD4 count of less than 5. PCR was positive for T. Cruzi.
Treatment¶
- Antiparasitic therapy (benznidazole or nifurtimox), plus antiretrovirals in reactivation disease
Differential diagnosis¶
| Differential Diagnosis | Distinguishing Feature |
|---|---|
| Toxoplasmosis | Multiple ring-enhancing lesions with eccentric target sign, favours basal ganglia and grey-white junction |
| Primary CNS lymphoma | Homogeneously enhancing periventricular lesion with restricted diffusion |
| Tuberculoma | Ring-enhancing lesion with central T2 hypointensity; often with basal meningitis |
| Cerebral abscess | Ring-enhancing lesion with marked central DWI restriction |
| Cerebral metastasis | Enhancing lesion at grey-white junction with extensive vasogenic oedema |
| Cardioembolic infarct | Multi-territory wedge-shaped cortical DWI restriction |
-
de Sousa et al. Chagas disease. 2024. Lancet (London, England) - Open in new tab. ↩