Cerebral Abscess¶
Summary
- Focal, purulent infection within the brain parenchyma
- Typically presents with headache, fever, and focal neurological deficits
- Imaging shows ring-enhancing lesion with surrounding oedema on CT/MRI1
Pathophysiology¶
- Caused by bacterial, fungal, or parasitic infections
- Three main routes of infection:
- Hematogenous spread (30-40%)
- Direct extension from contiguous infections (20-30%)
- Post-traumatic or post-surgical (10-15%)
- Progression through four stages:
- Early cerebritis (1-3 days)
- Late cerebritis (4-9 days)
- Early capsule formation (10-13 days)
- Late capsule formation (>14 days)
Demographics¶
- Incidence: 0.3-1.3 per 100,000 person-years
- More common in males (2:1 male-to-female ratio)
- Peak incidence in third and fourth decades of life
- Risk factors:
- Immunosuppression
- Congenital heart disease
- Chronic otitis media or sinusitis
- Dental infections
- Neurosurgical procedures
Diagnosis¶
- Clinical presentation:
- Headache (70-90%)
- Fever (45-70%)
- Focal neurological deficits (50-65%)
- Altered mental status (30-60%)
- Seizures (25-35%)
- Laboratory findings:
- Elevated white blood cell count
- Elevated C-reactive protein and erythrocyte sedimentation rate
- Lumbar puncture generally contraindicated due to risk of herniation
- Definitive diagnosis: culture of abscess contents
Imaging¶
- CT:
- Early stages: Ill-defined, low-density area with patchy enhancement
- Late stages: Well-defined, ring-enhancing lesion with surrounding oedema
- "Double ring sign": Hypodense centre with hyperdense rim and thin hypodense outer layer
- MRI:
- T1-weighted: Hypointense centre with isointense to hyperintense rim
- T2-weighted: Hyperintense centre with hypointense rim
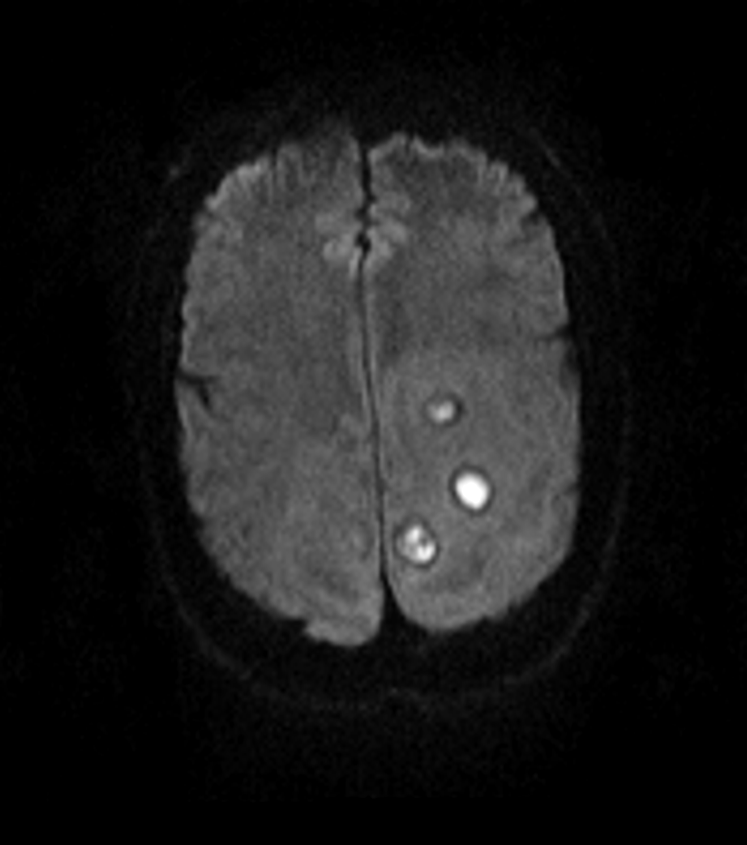
- DWI: Restricted diffusion in abscess cavity
- ADC: Low values in abscess cavity
- Contrast-enhanced: Ring enhancement with surrounding oedema
- Advanced techniques:
- MR spectroscopy: Elevated lactate, lipids, and amino acids
- Perfusion imaging: Low relative cerebral blood volume in abscess cavity
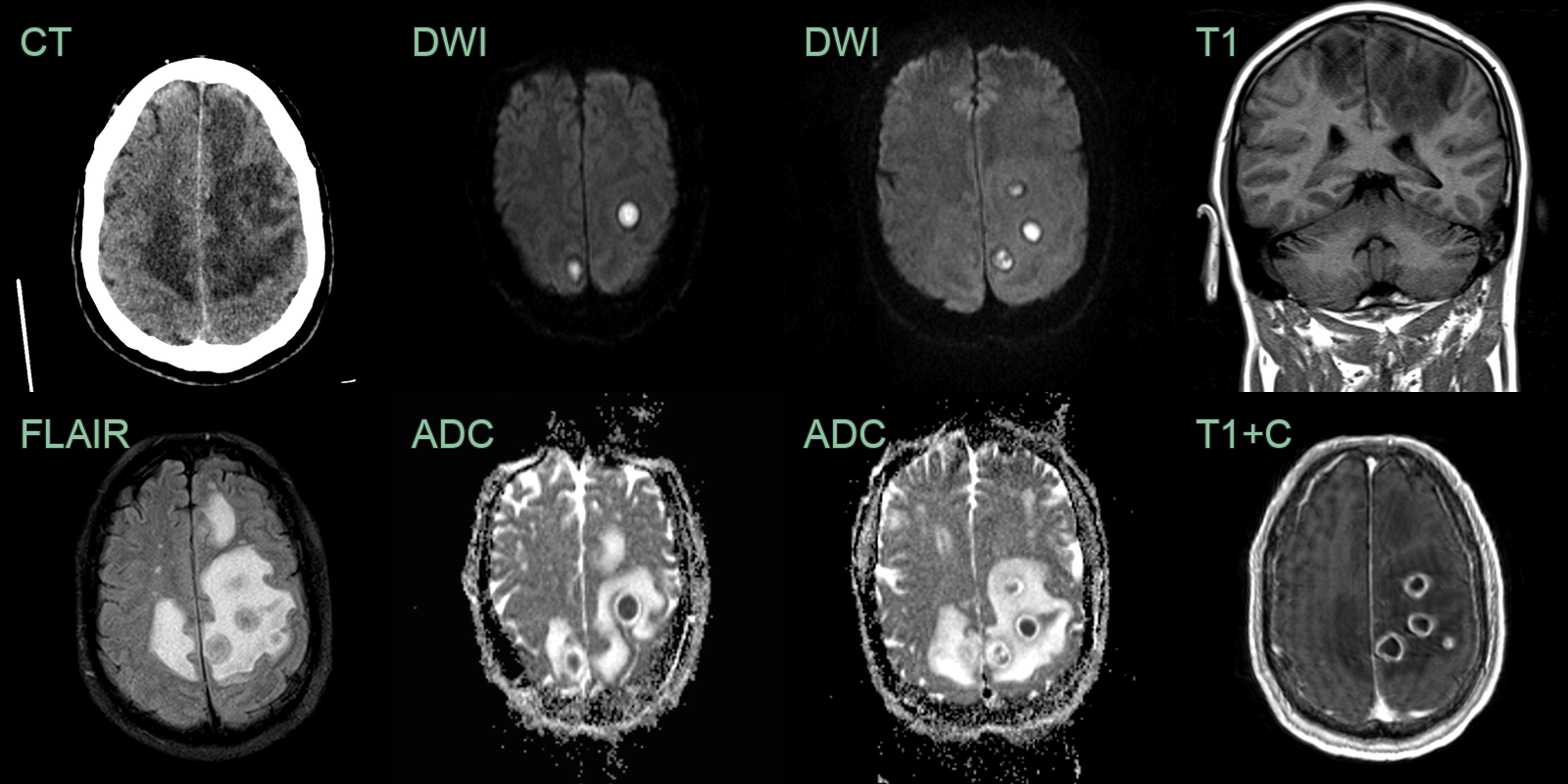
- A 50-year-old patient presented with a three-day history of fevers after a tonic-clonic seizure (three months after extensive dental work).
- Imaging showed many ring-enhancing lesions, with central diffusion restriction, surrounded by vasogenic oedema.
Treatment¶
- Prolonged targeted antibiotics with stereotactic aspiration or excision for larger lesions
- Serial imaging to confirm resolution
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Glioblastoma | Irregular ring enhancement on contrast-enhanced MRI; less restricted diffusion on DWI |
| Metastatic brain tumour | Multiple lesions; known primary cancer; smoother enhancement ring |
| Cerebral infarction | Follows vascular territory; no ring enhancement in acute phase |
| Toxoplasmosis | Multiple small lesions; HIV or immunocompromised status; positive serology |
| Tuberculoma | Solid nodular enhancement; concurrent pulmonary findings; positive TB tests |
| Demyelinating lesion | Incomplete ring sign; periventricular white matter involvement |
| Neurocysticercosis | Multiple cystic lesions; calcifications; travel history to endemic areas |
| Fungal infection | Irregular thick-walled lesions; immunocompromised status; CSF fungal culture |
| Subacute haematoma | Haemosiderin rim on T2*; history of trauma or coagulopathy |
| Radiation necrosis | History of radiation therapy; delayed onset after treatment |
-
Cossu et al. Cerebral abscess after neuro-vascular embolization: Own experience and review of the literature. 2017. Acta neurochirurgica - Open in new tab. ↩