Dural Arteriovenous Fistula¶
Summary
- Abnormal connection between dural arteries and venous sinuses or cortical veins
- Presents with pulsatile tinnitus, headache, or intracranial haemorrhage
- Diagnosed by catheter angiography; treated with endovascular embolisation or surgery1
Pathophysiology¶
- Acquired lesions resulting from:
- Venous sinus thrombosis
- Trauma
- Surgery
- Hypercoagulable states
- Classified by Cognard or Borden systems based on venous drainage pattern
- Increased risk of intracranial haemorrhage with cortical venous drainage
Demographics¶
- Incidence: 0.15-0.29 per 100,000 person-years
- Peak age: 50-60 years
- Slight female predominance
- Higher incidence in postmenopausal women and pregnancy
Diagnosis¶
- Clinical presentation:
- Pulsatile tinnitus
- Headache
- Intracranial haemorrhage
- Seizures
- Neurological deficits
- Bruit on auscultation over mastoid or orbit
- Catheter angiography: gold standard for diagnosis and classification
Imaging¶
- CT:
- Nonspecific findings
- May show dilated vessels, venous sinus thrombosis, or haemorrhage
- CT angiography:
- Demonstrates abnormal arterial feeders and early venous filling
- Limited in detecting small fistulas
- MRI:
- Flow voids representing enlarged vessels
- T2 hyperintensity in white matter (venous congestion)
- Susceptibility-weighted imaging: prominent cortical veins
- MR angiography:
- Time-of-flight and contrast-enhanced techniques
- Shows abnormal arterial feeders and early venous filling
- Catheter angiography:
- Definitive diagnosis and classification
- Identifies arterial feeders, fistula location, and venous drainage pattern
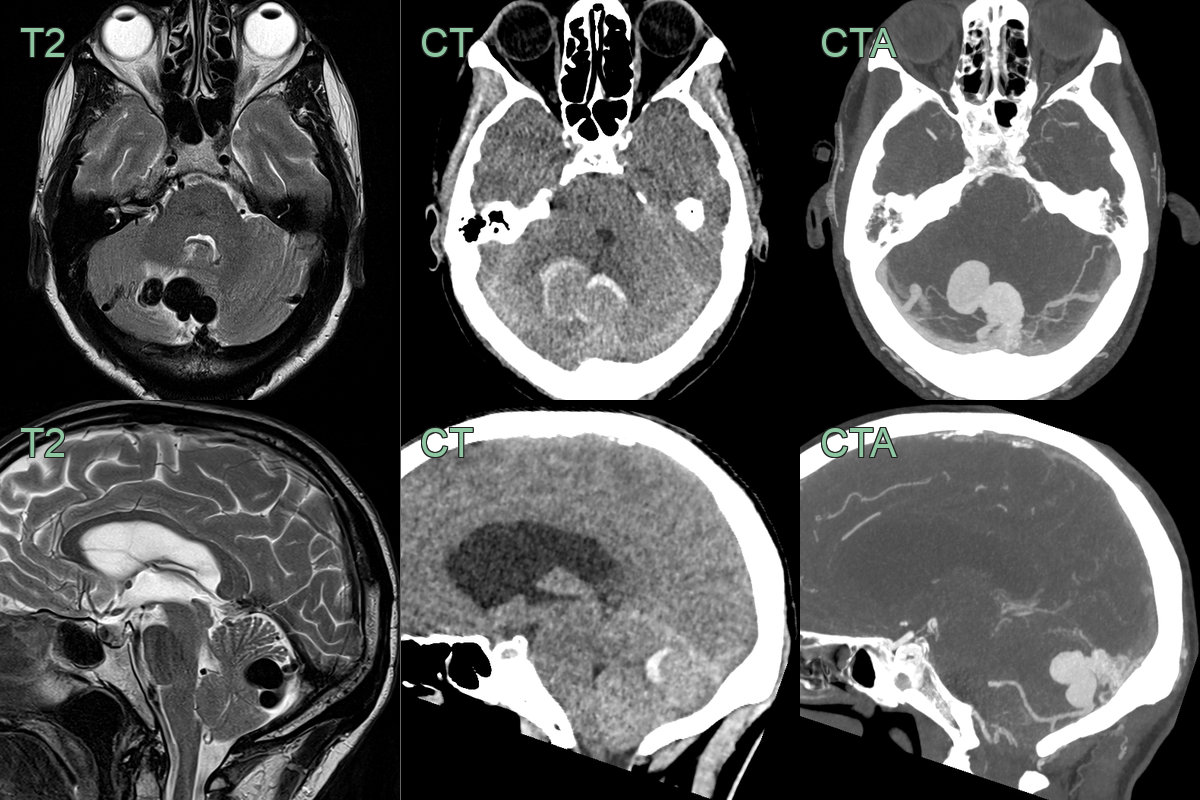
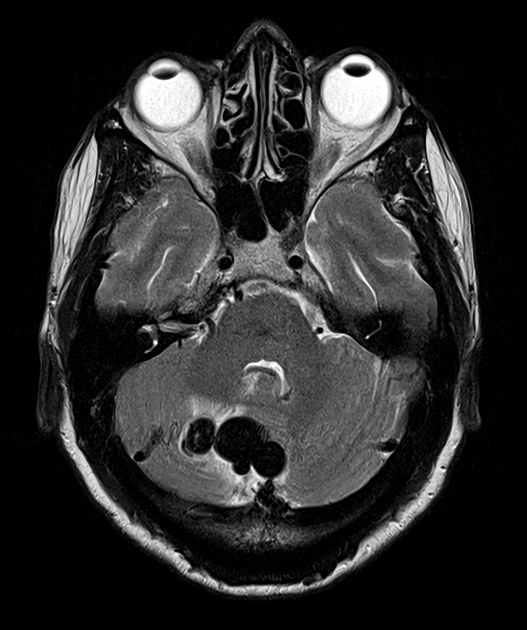
- A 60-year-old patient presented with headache.
- An MRI on admission showed a dilated vessel in the posterior fossa with a rim of oedema within the cerebellum.
- Immediately after the MRI, the patient's headache worsened and a CTA showed haemorrhage around the dural arteriovenous fistula that was supplied by the PICA.
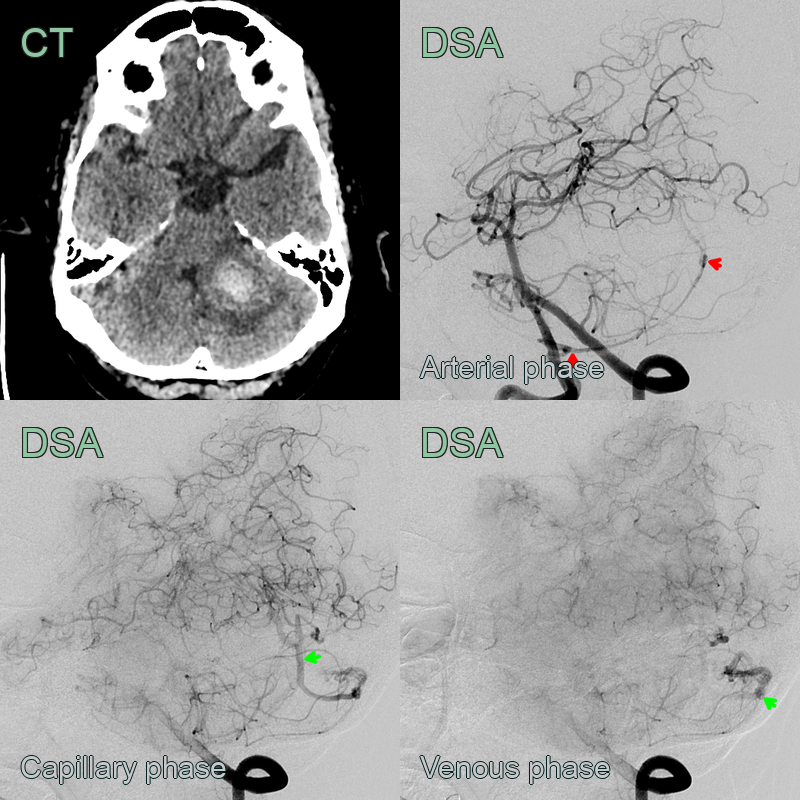
- A 60-year-old patient presented with headache and ataxia.
- The arterial phase of the DSA showed an abnormal vessel arising from the PICA draining into a dilated vein.
Treatment¶
- Cortical venous drainage (Cognard IIb+) is the key indication for treatment, usually by endovascular (often transvenous) embolisation
- Low-grade fistulas without cortical reflux may be observed
Differential diagnosis¶
| Imaging differential | Differentiating feature |
|---|---|
| Arteriovenous malformation | Parenchymal nidus supplied by pial arteries, rather than a direct dural shunt |
| Pial arteriovenous fistula | Direct artery-to-vein shunt within the parenchyma, pial rather than dural supply |
| Carotid-cavernous fistula | Shunt into the cavernous sinus with a dilated superior ophthalmic vein and proptosis |
| Dural venous sinus thrombosis | Sinus filling defect without arterial feeders (though it can cause a fistula) |
| Vascular tumour (e.g. haemangiopericytoma) | Enhancing dural mass rather than a network of shunting vessels |
-
Alkhaibary et al. Intracranial dural arteriovenous fistula: a comprehensive review of the history, management, and future prospective. 2023. Acta neurologica Belgica - Open in new tab. ↩