Facial Neurovascular Conflict¶
Summary
- Neurovascular compression of the facial nerve (CN VII) at the root exit zone causing hemifacial spasm
- Results from vascular loop compression, typically by anterior inferior cerebellar artery (AICA) or posterior inferior cerebellar artery (PICA)
- High-resolution MRI with CISS/FIESTA sequences demonstrates vascular contact at the cisternal segment of CN VII1
Pathophysiology¶
- Mechanism of compression
- Arterial pulsations cause chronic irritation of facial nerve at root exit zone (REZ)
- REZ is transition zone between central and peripheral myelin (2-3mm from brainstem)
- Most vulnerable area due to lack of epineurium
- Pathologic changes
- Demyelination at compression site
- Ephaptic transmission between adjacent nerve fibres
- Hyperexcitability of facial nerve nucleus
- Offending vessels
- AICA (most common - 40-50%)
- PICA (30-40%)
- Vertebral artery (10%)
- Basilar artery dolichoectasia (rare)
- Venous compression (extremely rare)
Demographics¶
- Incidence
- 11 per 100,000 population
- Accounts for primary hemifacial spasm in >95% of cases
- Age
- Peak incidence: 5th-6th decade
- Mean age at onset: 45-50 years
- Rare in patients <30 years
- Gender
- Female predominance (2:1 ratio)
- Laterality
- Left side more commonly affected (60%)
- Bilateral involvement rare (<1%)
Diagnosis¶
- Clinical presentation
- Involuntary, intermittent tonic-clonic contractions of facial muscles
- Typically begins in orbicularis oculi muscle
- Progresses caudally to involve lower face
- Exacerbated by stress, fatigue, voluntary facial movements
- Persists during sleep (distinguishes from blepharospasm)
- Electrophysiology
- Abnormal muscle response on EMG
- Lateral spread response on nerve conduction studies
- Synkinesis between different facial nerve branches
- Differential diagnosis
- Secondary hemifacial spasm (tumour, AVM, aneurysm)
- Facial myokymia
- Blepharospasm
- Facial tics
- Post-Bell's palsy synkinesis
Imaging¶
- High-resolution 3D heavily T2-weighted sequences (CISS/FIESTA), ≤1 mm, through the CPA are the mainstay
- Show a vessel contacting, indenting or displacing CN VII at the root exit zone; perpendicular contact is most significant
- TOF-MRA identifies the offending vessel and excludes an aneurysm or malformation
- Contrast is used mainly to exclude an enhancing mass (schwannoma, meningioma)
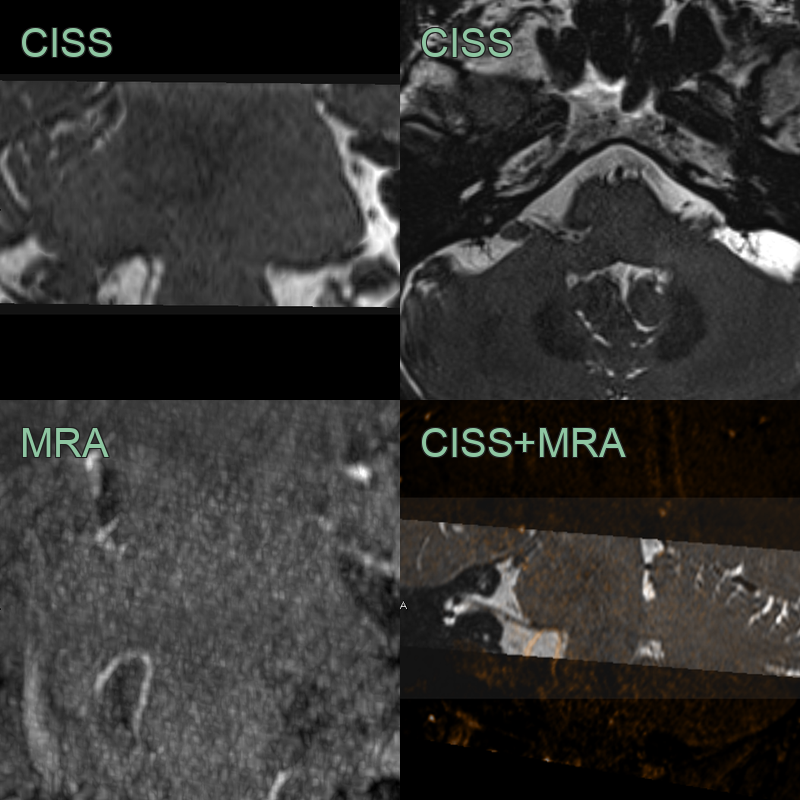
- A patient presenting with right hemifacial spasm has an MRI showing contact between the attached segment of the facial nerve and a superiorly looping PICA.
Treatment¶
- Medical therapy (carbamazepine, botulinum toxin); microvascular decompression is definitive for refractory cases
Differential diagnosis (secondary causes of hemifacial spasm at the CN VII root exit zone)¶
| Imaging differential | Differentiating feature |
|---|---|
| Facial schwannoma | Enhancing fusiform mass along the nerve rather than a vascular loop |
| Meningioma | Enhancing dural-based CPA mass with a dural tail |
| Epidermoid cyst | Diffusion-restricting insinuating CPA lesion |
| Vertebrobasilar dolichoectasia / aneurysm | Ectatic or aneurysmal vessel contacting the REZ |
-
Jesuthasan et al. Hemifacial spasm: an update on pathophysiology, investigations and management. 2025. Journal of neurology - Open in new tab. ↩