Epidermoid Cyst¶
Summary
- Benign, slow-growing congenital lesion containing keratin and cholesterol
- Typically in the cerebellopontine angle or parasellar region, insinuating around and encasing vessels and nerves
- Follows CSF signal but shows characteristic restricted diffusion and incomplete FLAIR suppression1
Pathophysiology¶
- Derived from ectoderm trapped during neural tube closure (3rd-5th week of embryogenesis)
- Lined by stratified squamous epithelium producing keratin debris
- Slow growth rate (1-2 mm/year) due to desquamation of epithelial cells
Demographics¶
- Accounts for 0.2-1.8% of all intracranial tumours
- Male to female ratio: 1.3:1
- Peak incidence: 20-40 years of age
- Rare in children (<5% of cases)
Diagnosis¶
- Often asymptomatic and discovered incidentally
- When symptomatic:
- Headache (most common)
- Cranial nerve deficits (especially CN V, VII, VIII)
- Cerebellar signs
- Seizures (if supratentorial)
- Rarely, can rupture causing chemical meningitis
Imaging¶
- CT:
- Hypodense, well-circumscribed lesion
- No enhancement with contrast
- Calcifications in 10-25% of cases
- MRI:
- T1: Hypointense to isointense
- T2: Hyperintense
- FLAIR: incomplete/heterogeneous suppression ("dirty CSF"), unlike an arachnoid cyst
- DWI: marked restriction — the key diagnostic feature
- No enhancement with gadolinium
- Insinuates through cisterns and encases vessels/nerves rather than displacing them
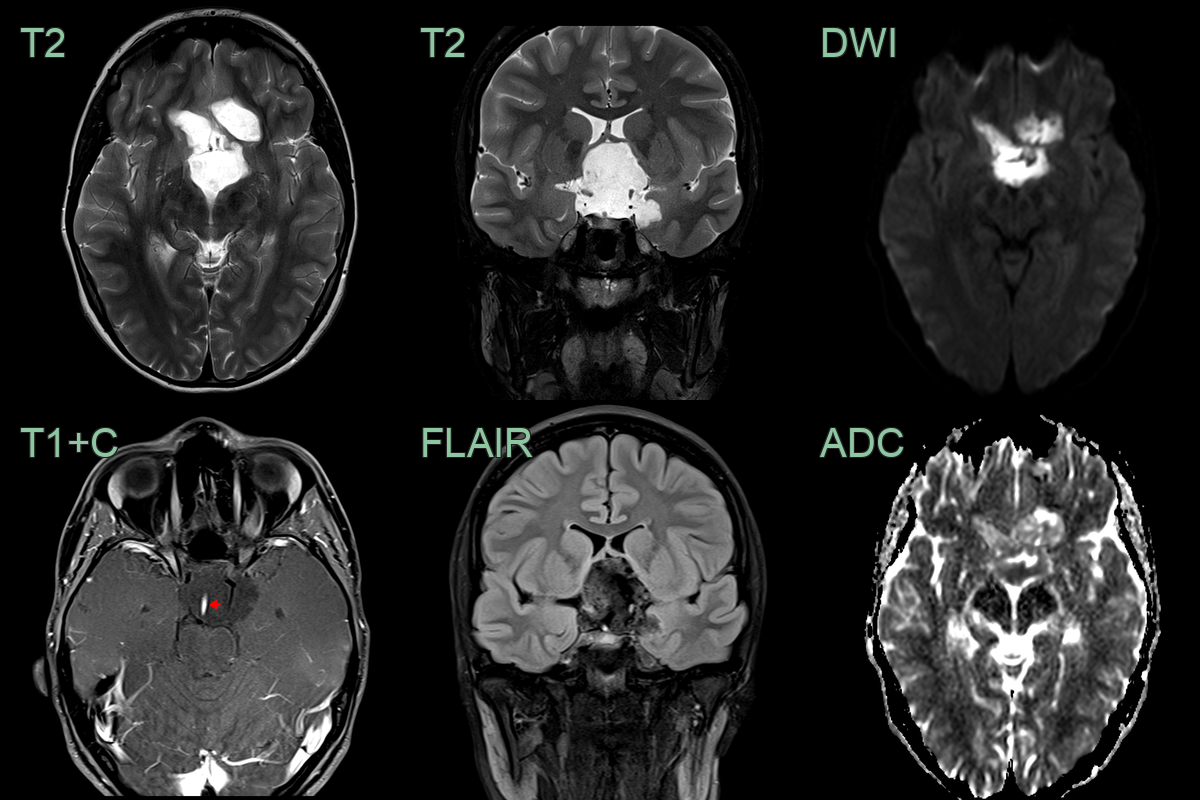
- 25-year-old patient presented with headache.
- MRI showed a diffusion-restricting non-enhancing suprasellar lesion that encased arteries and the infundibular stalk.
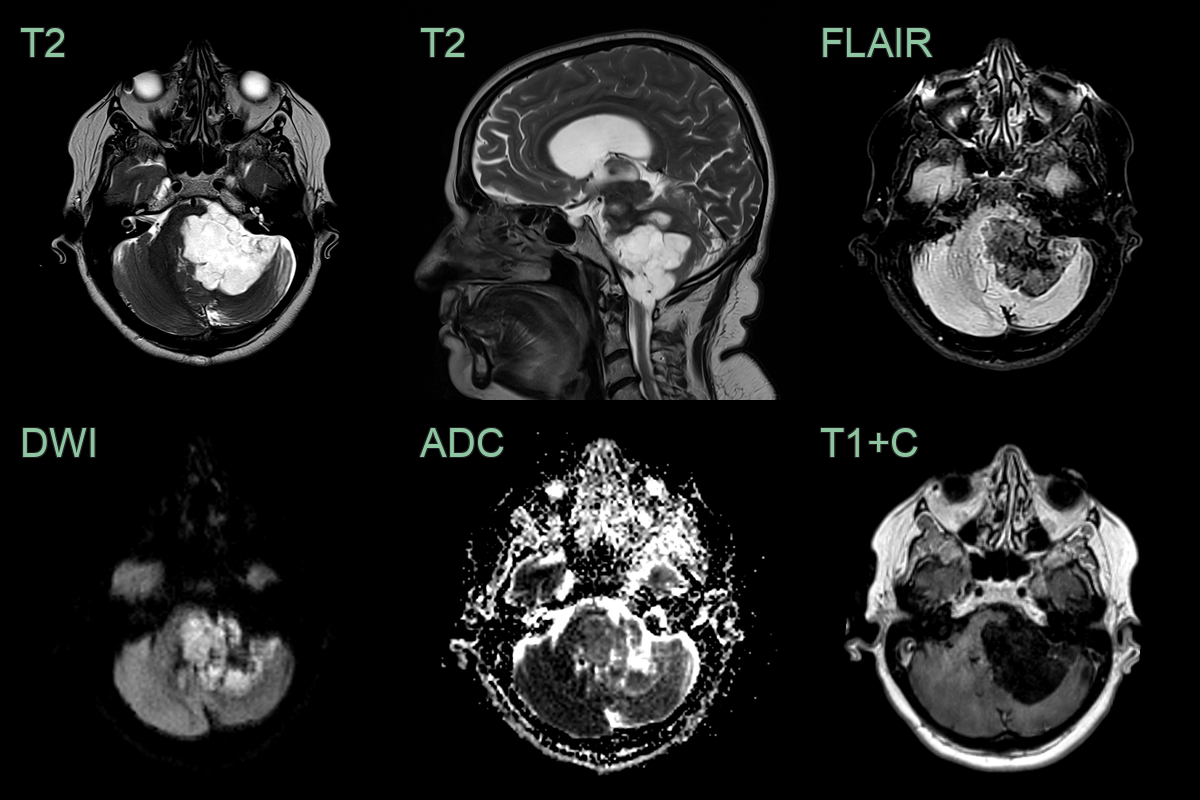
- 60-year-old patient present with ataxia and poor left-sided hearing.
- MRI showed a T2-hyperintense non-enhancing lobulated lesion with low ADC values in the left side of the posterior fossa, encasing the 7th and 8th nerve complexes.
- There was significant mass effect on the cerebellum (presumably relevant to the ataxia) but there was no oedema, indicating that this lesion has grown slowly.
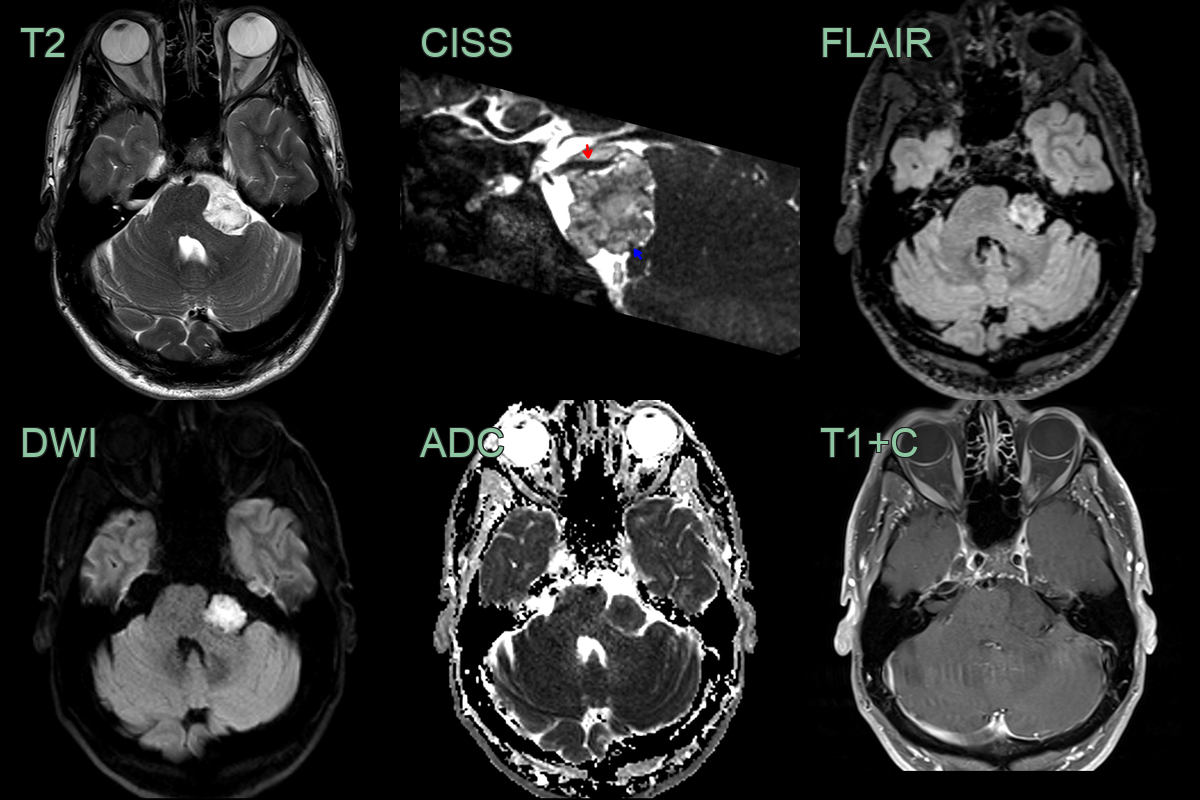
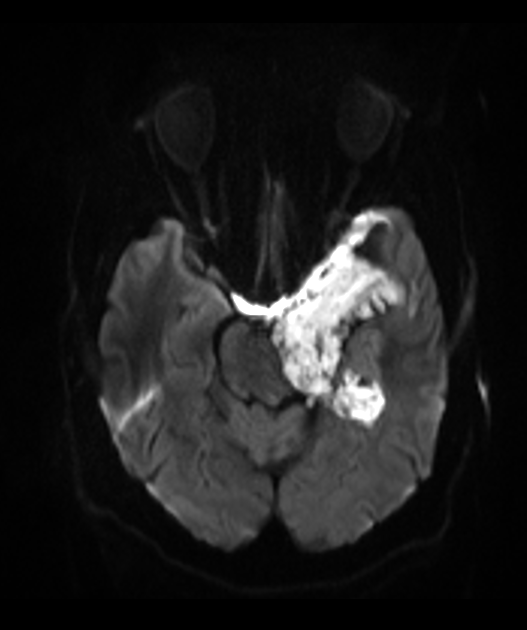
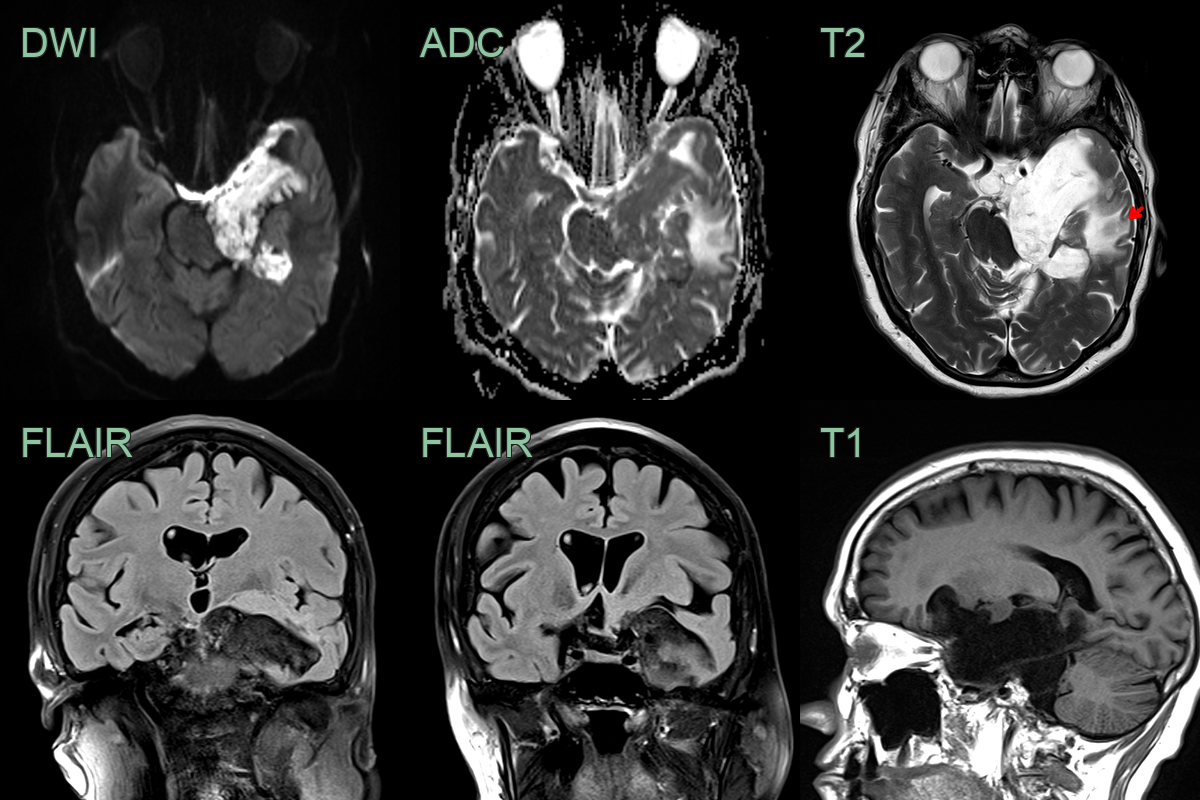
- 40-year-old patient presented with facial weakness and paraesthesia.
- MRI showed a 2.2 cm lesion in the left cerebellopontine angle cistern that caused diffusion restriction.
- The lesion displaced the trigeminal nerve (red arrow) and facial nerve (blue arrow).
Treatment¶
- Observation for asymptomatic lesions
- Surgical resection for symptomatic cases:
- Goal: maximal safe resection
- Complete resection challenging due to adherence to neurovascular structures
- Subtotal resection acceptable to preserve neurological function
- Gamma Knife radiosurgery:
- Alternative for residual or recurrent tumours
- Limited effectiveness due to slow growth rate
- Regular follow-up with MRI recommended due to potential for recurrence
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Dermoid cyst | Contains T1-hyperintense fat |
| Arachnoid cyst | No diffusion restriction on MRI |
| Neurenteric cyst | Typically located ventral to the brainstem or spinal cord; T1 hyperintense |
| Abscess | Surrounding oedema and contrast enhancement |
| Cholesteatoma | Typically found in the middle ear or mastoid |
-
Spinato et al. Giant Epidermoid Cyst of Posterior Fossa-Our Experience and Literature Review. 2021. Dose-response : a publication of International Hormesis Society - Open in new tab. ↩