Neurenteric Cyst¶
Summary
- Rare congenital malformation of the central nervous system
- Endodermal-derived cysts lined with mucin-secreting epithelium
- Typically located in the posterior fossa or spinal canal, often ventral to the spinal cord1
Pathophysiology¶
- Believed to result from incomplete separation of endoderm and ectoderm during embryogenesis
- Persistence of the neurenteric canal, leading to communication between the primitive endoderm and ectoderm
- Cysts are lined with columnar or cuboidal epithelium, often with mucin-producing goblet cells
- May contain components of respiratory or gastrointestinal epithelium
Demographics¶
- Rare lesions, accounting for 0.7-1.3% of all spinal cord tumours
- More common in males (M:F ratio 2:1)
- Usually diagnosed in the first two decades of life
- Spinal neurenteric cysts are more common than intracranial ones
Diagnosis¶
- Clinical presentation varies depending on location and size:
- Spinal: myelopathy, radiculopathy, or local pain
- Intracranial: headache, cranial nerve deficits, or symptoms of mass effect
- Histopathological examination is required for definitive diagnosis
- Differential diagnosis includes:
- Arachnoid cyst
- Epidermoid cyst
- Dermoid cyst
- Ependymal cyst
Imaging¶
- MRI is the imaging modality of choice:
- T1-weighted: variable signal intensity, often isointense to CSF
- T2-weighted: hyperintense signal, may show internal septations
- FLAIR: usually suppressed, similar to CSF
- Contrast enhancement: typically absent or minimal
- CT findings:
- Hypodense, well-circumscribed lesion
- May show calcifications in rare cases
- Spinal X-rays may show:
- Widening of the spinal canal
- Scalloping of vertebral bodies
- Associated vertebral anomalies (e.g., hemivertebrae, butterfly vertebrae)
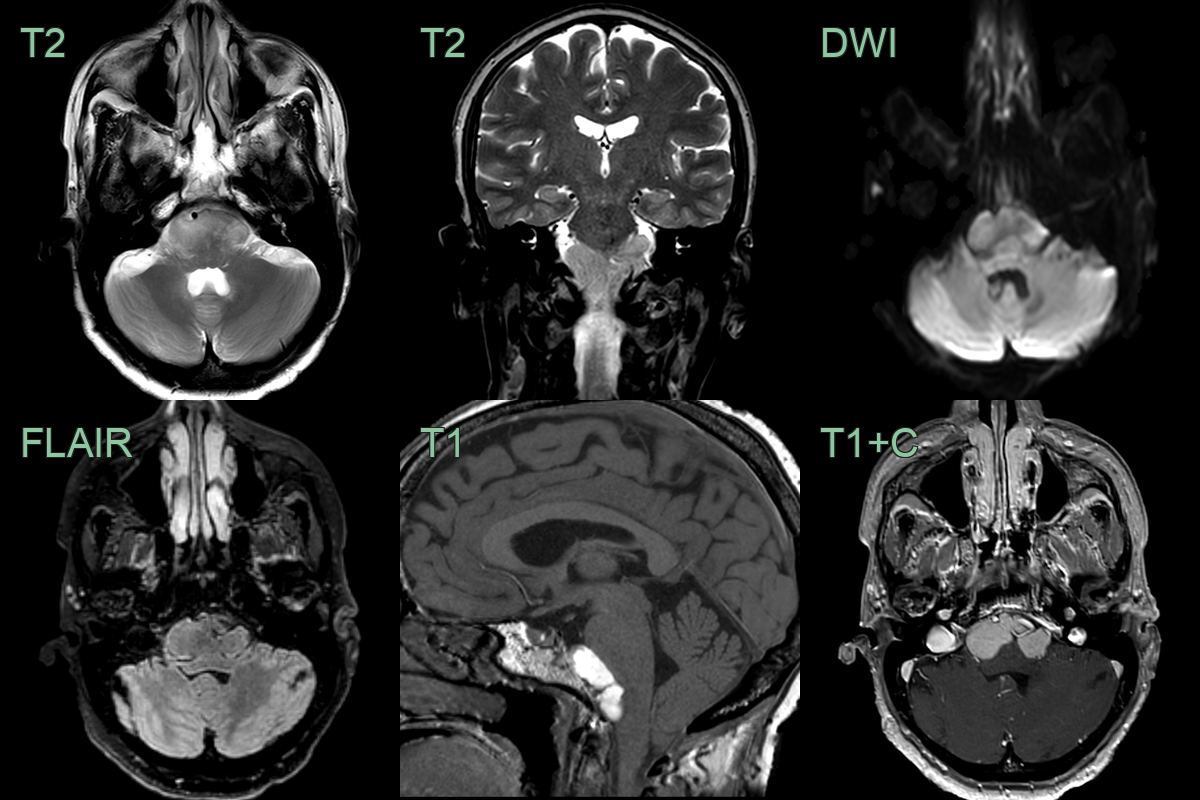
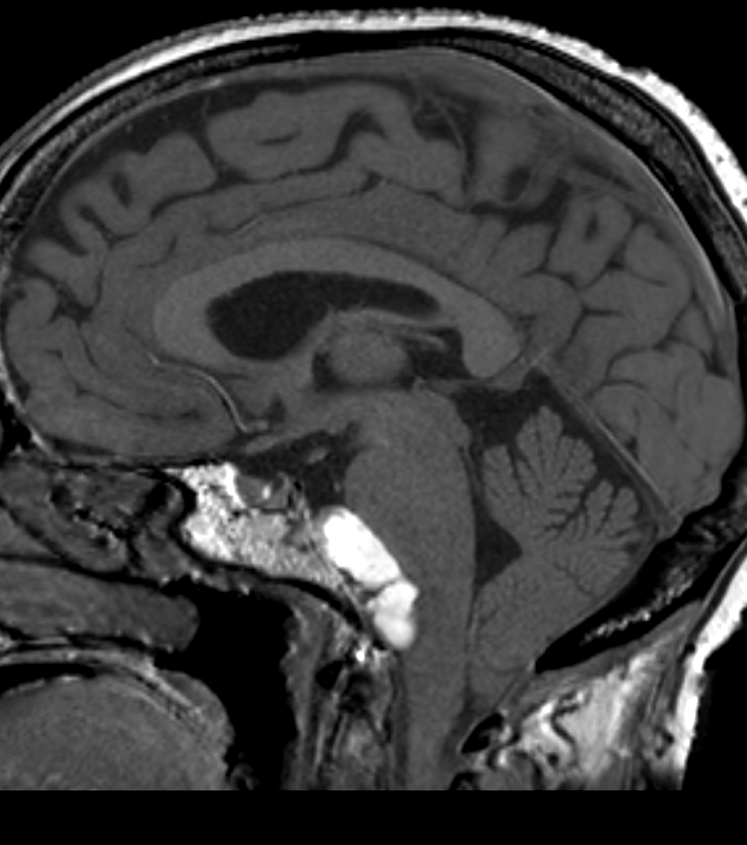
- An incidental lesion in a patient who had an MRI after a suspected TIA.
- A lobulated lesion causing mild mass effect on the brainstem was T1-hyperintense and isointense on fat-suppressed FLAIR (the latter making a lipoma less likely).
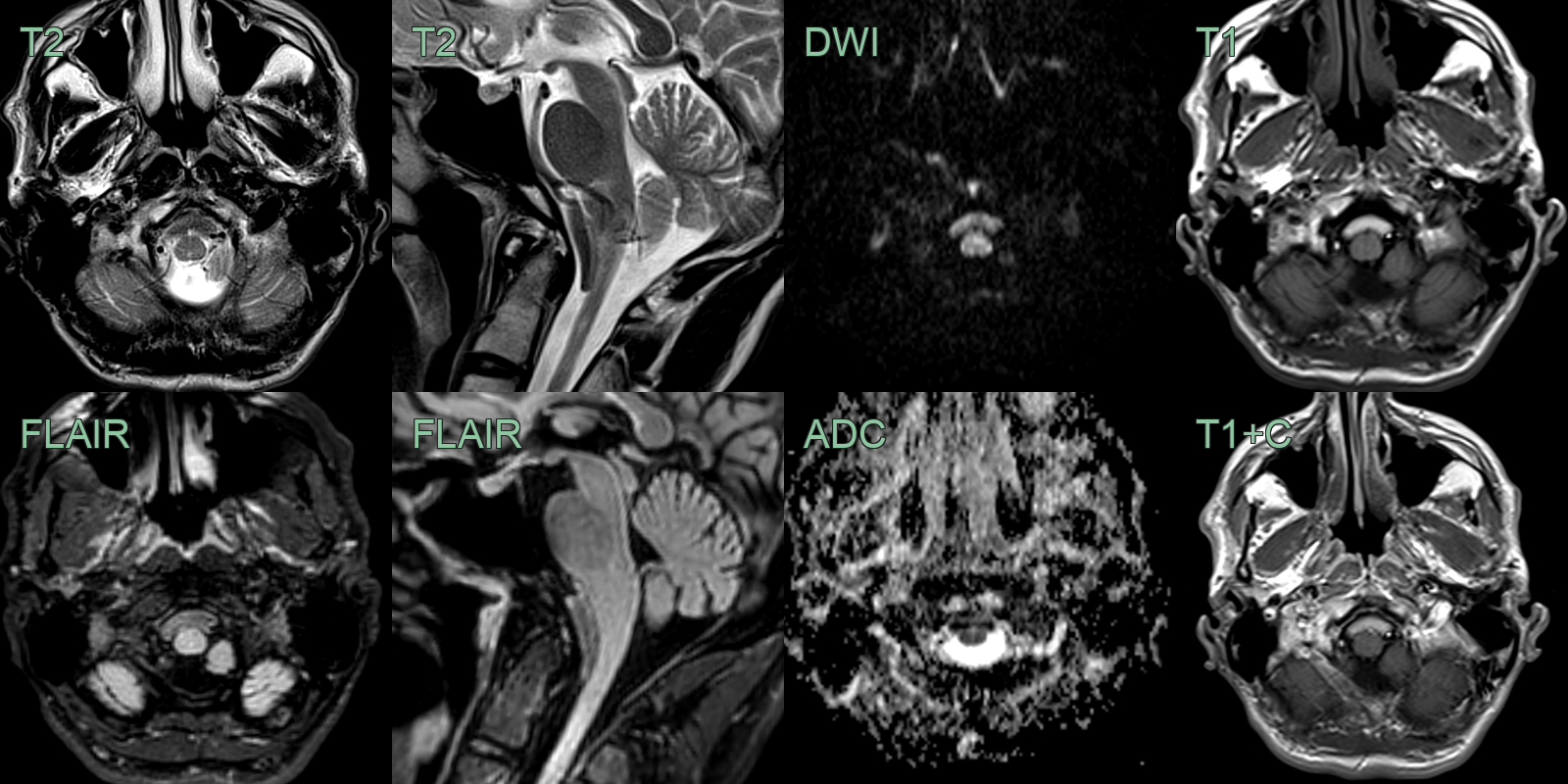
- A 50-year-old patient with MS had an incidental lesion in the premedullary space that had not changed in over a decade.
- Consistent with a neurenteric cyst, the lesion was T1-hyperintense, T2-hypointense and did not enhance.
Treatment¶
- Surgical resection for symptomatic lesions. A non-enhancing, often T1-hyperintense cyst sitting ventral to the brainstem or cord is the classic appearance
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Arachnoid Cyst | Lacks enhancement and does not contain mucoid or proteinaceous material |
| Epidermoid Cyst | Demonstrates diffusion restriction on MRI |
| Dermoid Cyst | Contains fat and calcifications |
| Pilocytic Astrocytoma | Enhances with contrast and has solid components |
| Ependymoma | Typically has calcifications and heterogeneous enhancement |
| Choroid Plexus Cyst | Located within the ventricles and has CSF-like signal |
| Colloid Cyst | Typically located in the third ventricle and has high protein content |
| Rathke's Cleft Cyst | Located in the sella turcica or suprasellar region |
| Enterogenous Cyst | Similar features, but typically found in the posterior mediastinum |
| Teratoma | Contains multiple tissue types including fat, calcifications, and soft tissue |
-
Visvanathan et al. Neurenteric cyst presenting with stridor and dysphagia: case report and literature review. 2015. Scottish medical journal - Open in new tab. ↩