HIV-associated myelopathy¶
Summary
- Progressive spastic paraparesis and sensory ataxia in HIV patients
- Vacuolar myelopathy of the spinal cord, predominantly affecting thoracic region
- MRI shows cord atrophy and T2 hyperintensity in posterior and lateral columns1
Pathophysiology¶
- Exact mechanism unclear, but likely multifactorial:
- Direct HIV infection of spinal cord cells
- Immune-mediated damage to myelin and axons
- Metabolic disturbances, including vitamin B12 deficiency
- Vacuolar changes in white matter, predominantly in lateral and posterior columns
- Axonal degeneration and demyelination
Demographics¶
- Occurs in 5-10% of HIV-infected individuals
- More common in advanced stages of HIV infection (CD4 count <200 cells/μL)
- Typically affects adults aged 30-50 years
- No significant gender or racial predilection
Diagnosis¶
- Clinical presentation:
- Gradual onset of lower limb weakness and spasticity
- Sensory ataxia and impaired vibration sense
- Urinary and bowel dysfunction
- Exclusion of other causes of myelopathy (e.g., compression, infection)
- CSF analysis: may show mild pleocytosis and elevated protein
- Serum vitamin B12 levels should be checked
Imaging¶
- MRI findings:
- Spinal cord atrophy, particularly in thoracic region
- T2 hyperintensity in posterior and lateral columns
- Symmetrical involvement, typically extending over multiple segments
- No contrast enhancement
- Differential diagnosis:
- Vitamin B12 deficiency myelopathy
- HTLV-1-associated myelopathy
- Primary progressive multiple sclerosis
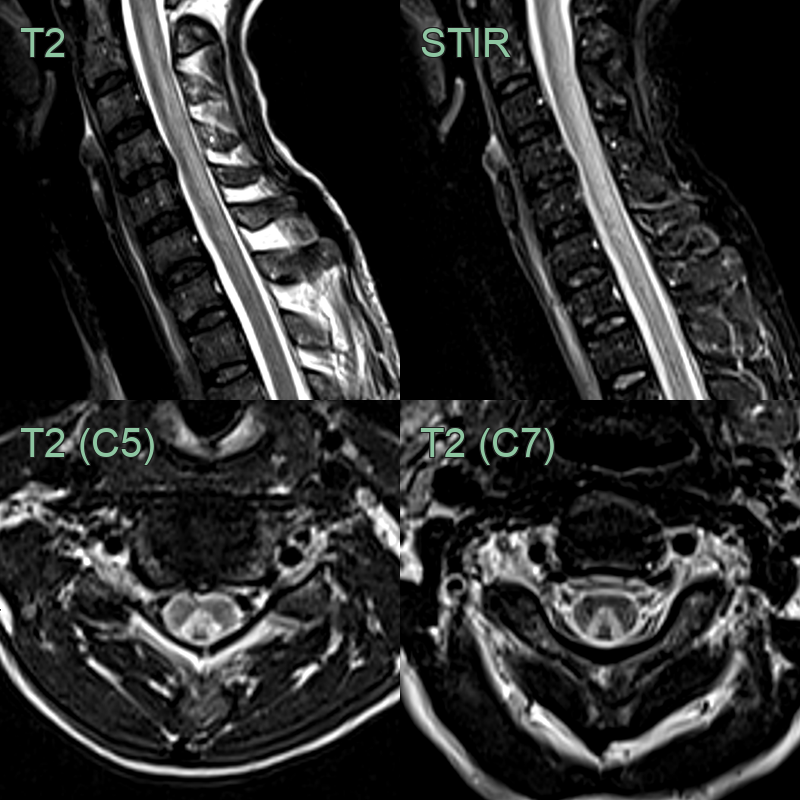
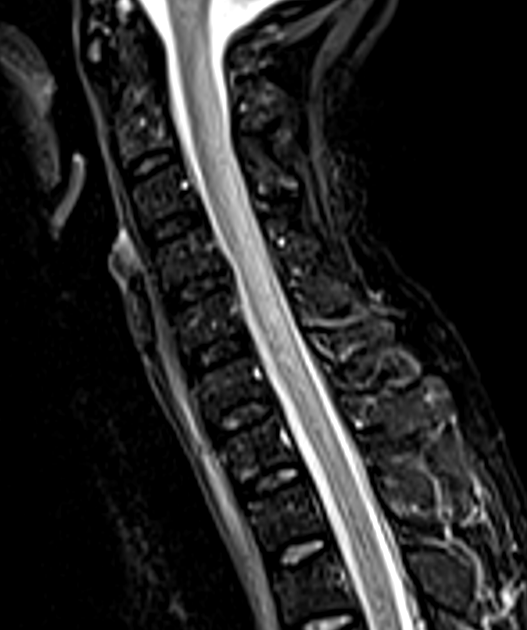
- 45-year-old patient presented with weakness and brisk upper limb reflexes. The patient had a recent diagnosis of HIV with a CD4 count of 10.
- MRI showed an "inverted V" pattern of high signal in the dorsal columns.
Treatment¶
- Antiretroviral therapy (may slow progression) with correction of any B12 deficiency and symptomatic management
Differential diagnosis (dorsal/lateral column myelopathy)¶
| Imaging differential | Differentiating feature |
|---|---|
| Subacute combined degeneration (B12) | Identical dorsal-column "inverted V" sign; distinguished by low B12/high methylmalonic acid |
| Copper deficiency myelopathy | Dorsal-column signal indistinguishable from SCD; history of bariatric surgery or zinc excess |
| HTLV-1 myelopathy | Thoracic cord atrophy with lateral column signal; positive HTLV-1 serology |
| Compressive myelopathy | Structural cord compression rather than symmetric column signal |
| NMOSD / transverse myelitis | Longitudinally extensive, often enhancing, central cord lesion |
-
Ayele et al. HIV-associated neurocognitive disorder and HIV-associated myelopathy in a patient with a preserved CD4, but high viral load-a rarely reported phenomenon: a case report and literature review. 2020. BMC infectious diseases - Open in new tab. ↩