Sacral Chordoma¶
Summary
- Rare malignant tumour arising from notochordal remnants, typically presenting in the sacrococcygeal region with insidious onset of lower back pain and neurological symptoms
- Characterised by locally aggressive growth with high recurrence rates, composed of physaliferous cells in a myxoid matrix
- Imaging demonstrates a large, lobulated, destructive sacral mass with high T2 signal intensity and heterogeneous enhancement1
Pathophysiology¶
- Arises from embryonic notochordal remnants along the axial skeleton
- Slow-growing but locally aggressive tumour with infiltrative growth pattern
- Composed of characteristic physaliferous (bubble-bearing) cells containing intracytoplasmic vacuoles
- Produces abundant extracellular myxoid matrix rich in mucopolysaccharides
- Expresses brachyury (T-gene product), a specific marker for notochordal differentiation
- Three histologic subtypes:
- Conventional (most common)
- Chondroid (better prognosis)
- Dedifferentiated (worst prognosis)
Demographics¶
- Accounts for 1-4% of all primary bone malignancies
- 50-60% occur in sacrococcygeal region
- Peak incidence in 5th-7th decades of life
- Male predominance (2:1 ratio)
- Rare in children and adolescents
- No specific ethnic predilection
- Familial chordoma accounts for <5% of cases (associated with duplications of brachyury gene)
Diagnosis¶
- Clinical presentation:
- Insidious onset of lower back pain (months to years)
- Constipation and bowel dysfunction
- Urinary incontinence or retention
- Lower extremity weakness and numbness
- Palpable presacral mass on rectal examination
- Laboratory findings:
- No specific serum markers
- Elevated alkaline phosphatase may be present
- Histopathology:
- Physaliferous cells with vacuolated cytoplasm
- Lobulated architecture separated by fibrous septa
- Myxoid stroma
- Immunohistochemistry positive for:
- Brachyury (highly specific)
- Cytokeratin
- EMA (epithelial membrane antigen)
- S100 protein
Imaging¶
- Plain radiography:
- Large lytic sacral mass with bone destruction
- Calcifications in 30-70% of cases
- Anterior soft tissue mass
- CT:
- Midline destructive sacral mass
- Mixed lytic and sclerotic bone changes
- Intratumoural calcifications
- Well-defined soft tissue component
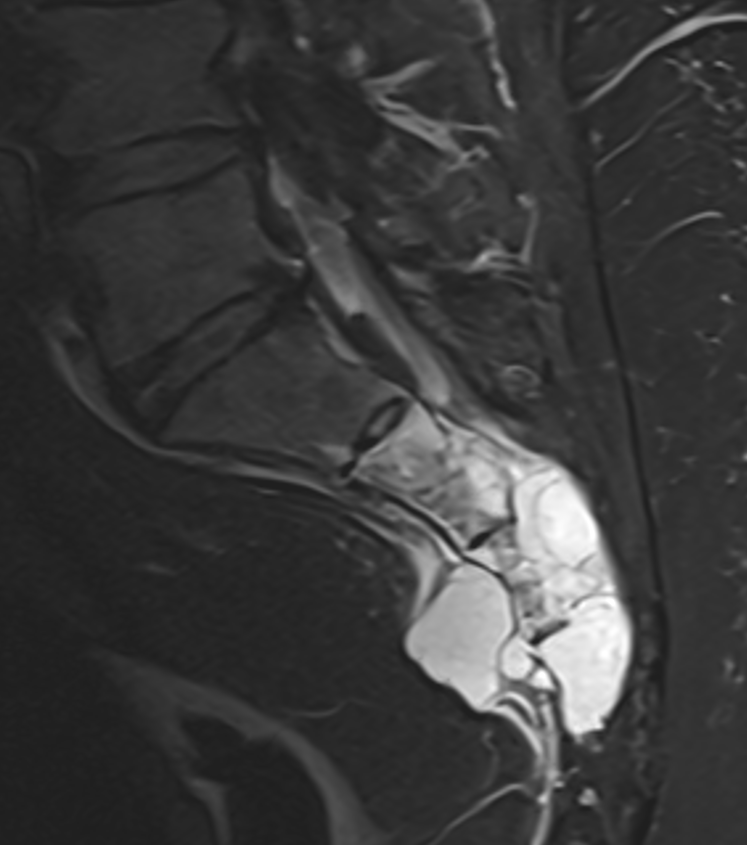
- MRI (modality of choice):
- T1: Hypointense to isointense relative to muscle
- T2: Markedly hyperintense (due to high mucin content)
- T1+C: Heterogeneous moderate enhancement with honeycomb pattern
- DWI: Variable restricted diffusion (ADC values typically intermediate)
- STIR: Hyperintense signal
- Sagittal imaging crucial for surgical planning
- Key imaging features:
- "Mushroom-shaped" configuration extending anteriorly into pelvis
- Lobulated contours with internal septations
- Involvement of multiple sacral segments
- Preservation of intervertebral disks (unlike metastases)
- PET/CT:
- Mild to moderate FDG uptake
- Useful for detecting metastases and recurrence
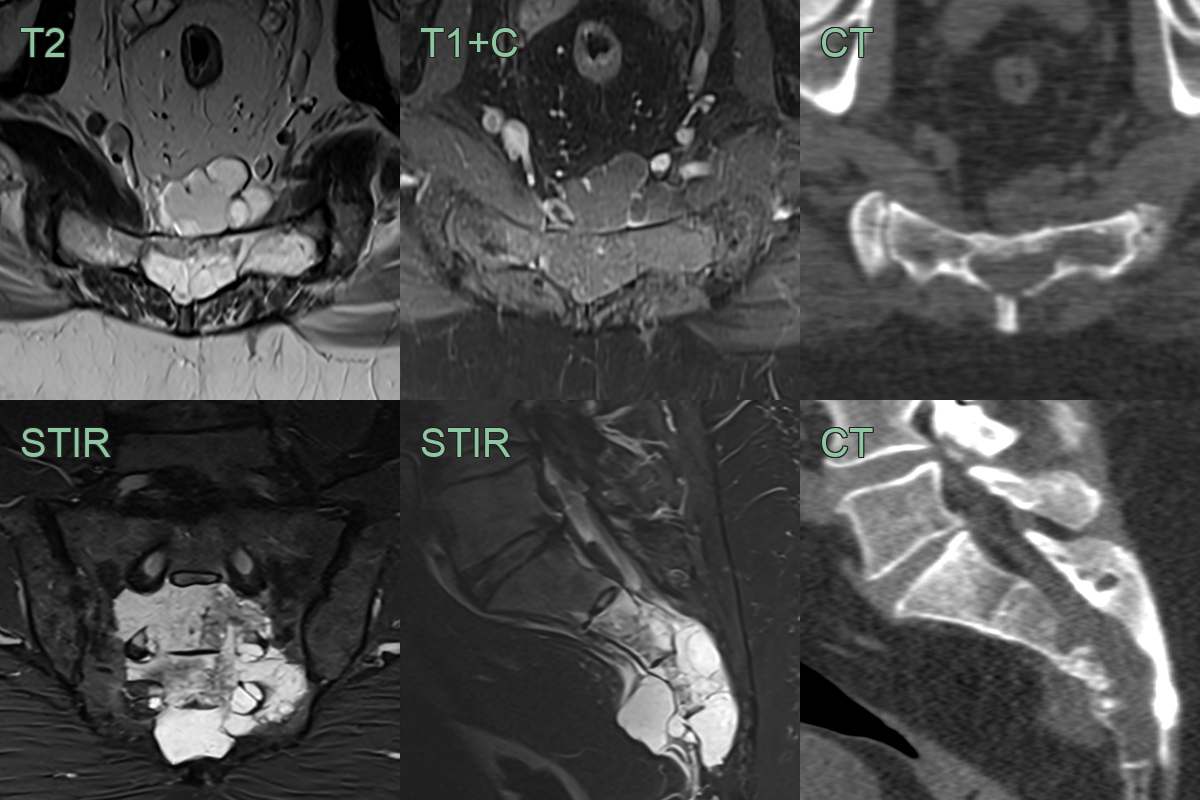
- A 50-year-old patient presented with sphincter disturbance and lower back pain.
- MRI showed a lobulated minimally enhancing T2-hyperintense lesion centred on the sacrum.
- CT showed loss of normal cortex.
- A CT-guided biopsy confirmed a sacral chordoma.
Treatment¶
- En bloc sacrectomy with wide margins is the mainstay, with adjuvant proton/carbon-ion radiotherapy; local recurrence is common. The very high T2 signal and preservation of disc spaces (unlike metastases) are key clues
Differential diagnosis¶
| Differential diagnosis | Differentiating feature |
|---|---|
| Giant cell tumour | Eccentric location, typically spares the midline; lacks calcifications; may have ABC-like areas with fluid-fluid levels |
| Chondrosarcoma | Often arises from sacroiliac joint; contains chondroid matrix with rings-and-arcs calcification pattern; lower T2 signal than chordoma |
| Metastases | Multiple lesions; usually more aggressive bone destruction; may have primary at another site on systemic imaging |
| Plasmacytoma/Myeloma | Punched-out lytic lesions on CT; typically spares disc spaces; diffuse marrow involvement on MRI |
| Neurogenic tumour | Arises from sacral foramina; expands neural foramen; smooth remodelling rather than destruction |
| Osteosarcoma | Aggressive periosteal reaction; osteoid matrix production; mixed lytic-sclerotic pattern |
| Ewing sarcoma | Permeative pattern with aggressive periosteal reaction; disproportionately large soft tissue mass; no calcifications |
| Lymphoma | Permeative pattern with relative preservation of cortex; soft tissue mass disproportionate to bone destruction |
| Aneurysmal bone cyst | Fluid-fluid levels on MRI; expansile with thin cortical shell; no solid enhancing component |
| Sacral meningioma | Intradural location; dural tail sign; homogeneous enhancement; no bone destruction |
-
Radaelli et al. The sacral chordoma margin. 2020. European journal of surgical oncology : the journal of the European Society of Surgical Oncology and the British Association of Surgical Oncology - Open in new tab. ↩