Skull Base Metastasis¶
Summary
- Skull base metastases are secondary malignant tumours that spread to the skull base from primary cancers elsewhere in the body
- Common primary sites include breast, lung, and prostate cancers
- Imaging plays a crucial role in diagnosis, with MRI being the modality of choice1
Pathophysiology¶
- Metastatic spread occurs via:
- Haematogenous route (most common)
- Direct extension from adjacent structures
- Perineural spread
- Skull base involvement can lead to:
- Cranial nerve palsies
- Intracranial extension
- Dural invasion
- Vascular compromise
Demographics¶
- Incidence increases with age, peak in 6th-7th decades
- Slightly more common in males
- Primary cancers most commonly associated:
- Breast (20-30%)
- Lung (10-20%)
- Prostate (10-15%)
- Others: renal, thyroid, melanoma
Diagnosis¶
- Clinical presentation:
- Cranial nerve palsies (most common)
- Headache
- Facial pain or numbness
- Diplopia
- Hearing loss
- Laboratory tests:
- Tumour markers (e.g., PSA, CA 15-3)
- Complete blood count
- Serum calcium levels
- Biopsy:
- Often required for definitive diagnosis
- CT or MRI-guided biopsy preferred
Imaging¶
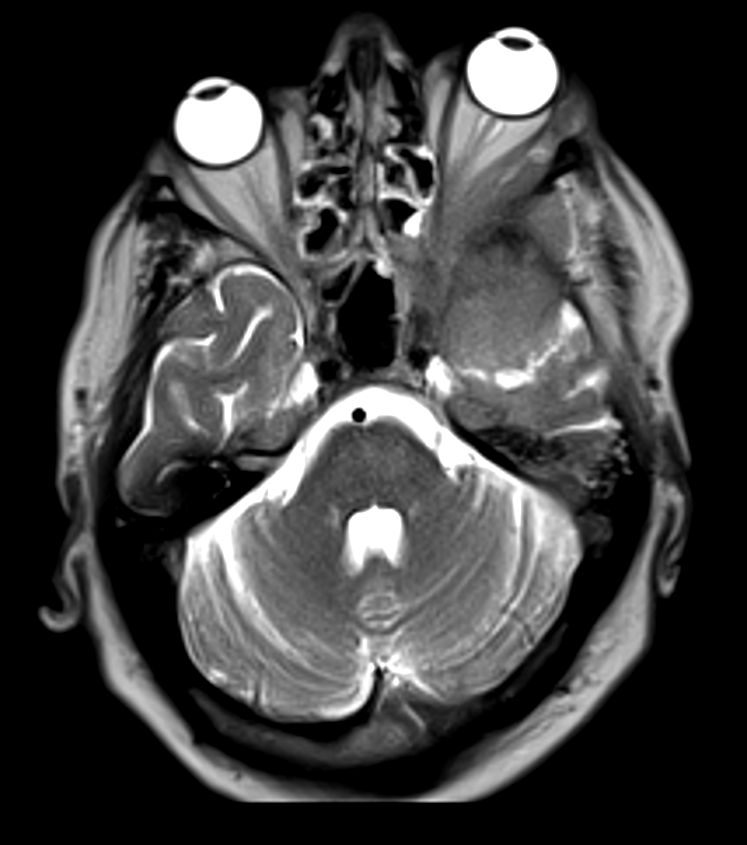
- MRI:
- Modality of choice
- T1-weighted images: hypointense lesions
- T2-weighted images: variable signal intensity
- Contrast-enhanced T1: heterogeneous enhancement
- Diffusion-weighted imaging: restricted diffusion
- CT:
- Complementary to MRI
- Bone window: lytic or sclerotic lesions
- Soft tissue window: mass effect, enhancement
- PET-CT:
- Useful for detecting primary tumour and other metastases
- High sensitivity for metabolically active lesions
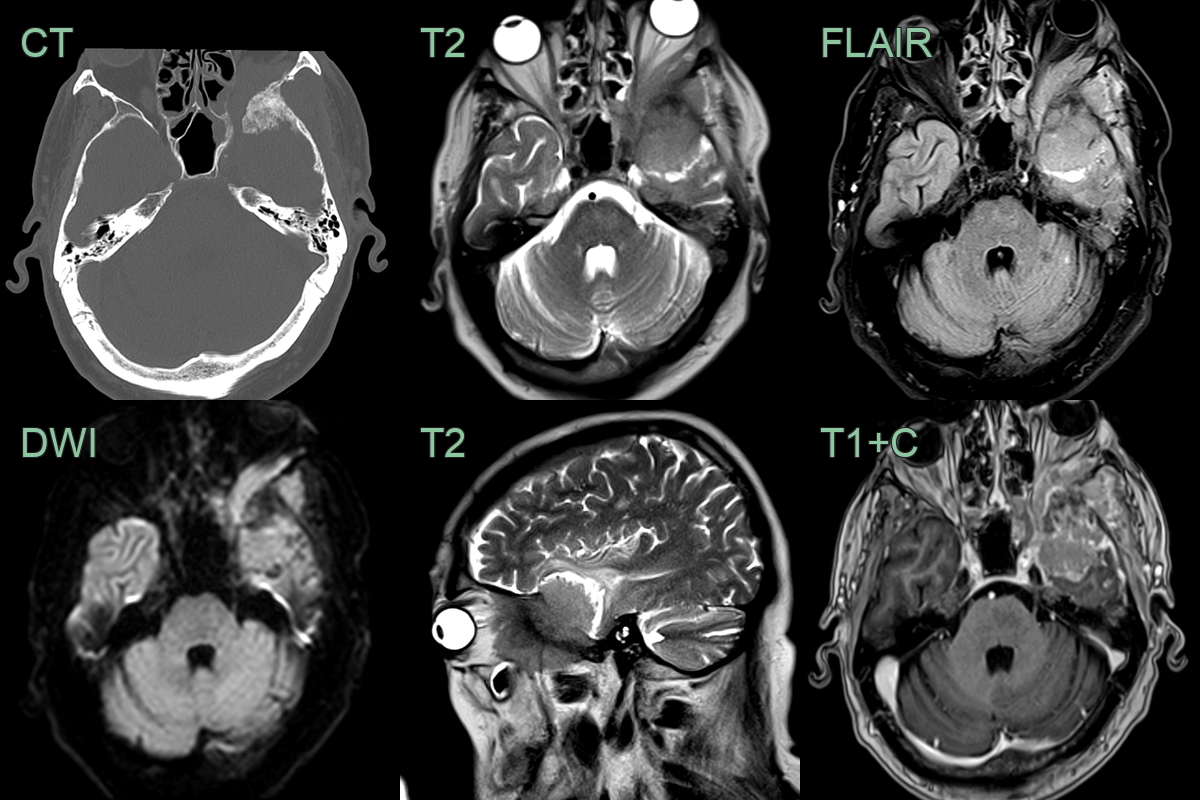
- A 70-year-old patient with known prostate cancer presented with headache and left-sided proptosis.
- CT showed expansion of the left sphenoid buttress surrounded by enhancing soft tissue.
- Biopsy revealed a prostate metastasis.
Treatment¶
- Palliative radiotherapy and systemic therapy directed at the primary; recognising the pattern of cranial neuropathy localises the affected skull base foramen
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Meningioma | Typically has a dural tail on MRI; often homogeneous enhancement |
| Pituitary adenoma | Centered in the sella turcica; homogeneously enhancing or cystic; no aggressive bone destruction |
| Chordoma | Midline lesion; typically involves the clivus; high T2 signal; "bubbly" lobular morphology |
| Schwannoma | Associated with cranial nerve course; often enhances homogeneously; smooth expansion of neural foramen |
| Nasopharyngeal carcinoma | Epicentre in nasopharynx with local invasion; skull base extension from below; cervical nodal metastases |
| Lymphoma | Homogeneous soft tissue mass; may have restricted diffusion on MRI; disproportionate soft tissue relative to bone destruction |
| Plasmacytoma | Single lytic lesion; "blown-out" cortex pattern; diffuse marrow involvement on MRI |
| Glomus tumour | Intense enhancement; "salt and pepper" appearance on MRI |
| Fibrous dysplasia | Ground-glass appearance on CT; low T1 and T2 signal on MRI |
-
Matsuno et al. Clinicopathological and molecular histochemical review of skull base metastasis from differentiated thyroid carcinoma. 2013. Acta histochemica et cytochemica - Open in new tab. ↩