Takayasu's Arteritis¶
Summary
- Chronic, large-vessel vasculitis primarily affecting the aorta and its major branches
- Characterised by granulomatous inflammation leading to vessel wall thickening, stenosis, and aneurysm formation
- Imaging findings include vessel wall thickening, luminal narrowing, and collateral vessel formation1
Pathophysiology¶
- Exact aetiology unknown, but likely autoimmune in nature
- Inflammatory process leads to:
- Granulomatous inflammation of vessel walls
- Intimal fibrosis and thickening
- Smooth muscle cell proliferation
- Eventual stenosis, occlusion, or aneurysm formation
- T-cell mediated immune response plays a crucial role in pathogenesis
Demographics¶
- Predominantly affects young women (80-90% of cases)
- Typical age of onset: 10-40 years
- More common in Asian populations, particularly Japan and Southeast Asia
- Incidence: 1-3 per million per year in North America and Europe
Diagnosis¶
- Based on clinical presentation, laboratory findings, and imaging studies
- American College of Rheumatology criteria (1990) include:
- Age at disease onset <40 years
- Claudication of extremities
- Decreased brachial artery pulse
- Blood pressure difference >10 mmHg between arms
- Bruit over subclavian arteries or aorta
- Arteriogram abnormality
- Laboratory findings:
- Elevated erythrocyte sedimentation rate (ESR)
- Elevated C-reactive protein (CRP)
- Anaemia of chronic disease
Imaging¶
- Conventional angiography:
- Gold standard for diagnosis
- Demonstrates luminal changes, stenosis, and occlusions
- CT angiography (CTA):
- Vessel wall thickening and enhancement
- Luminal narrowing or occlusion
- Collateral vessel formation
- MR angiography (MRA):
- Similar findings to CTA
- Advantages: no radiation exposure, better soft tissue contrast
- Ultrasound:
- Useful for carotid and subclavian artery assessment
- Demonstrates vessel wall thickening and stenosis
- 18F-FDG PET/CT:
- Detects active inflammation in vessel walls
- Useful for monitoring disease activity and treatment response
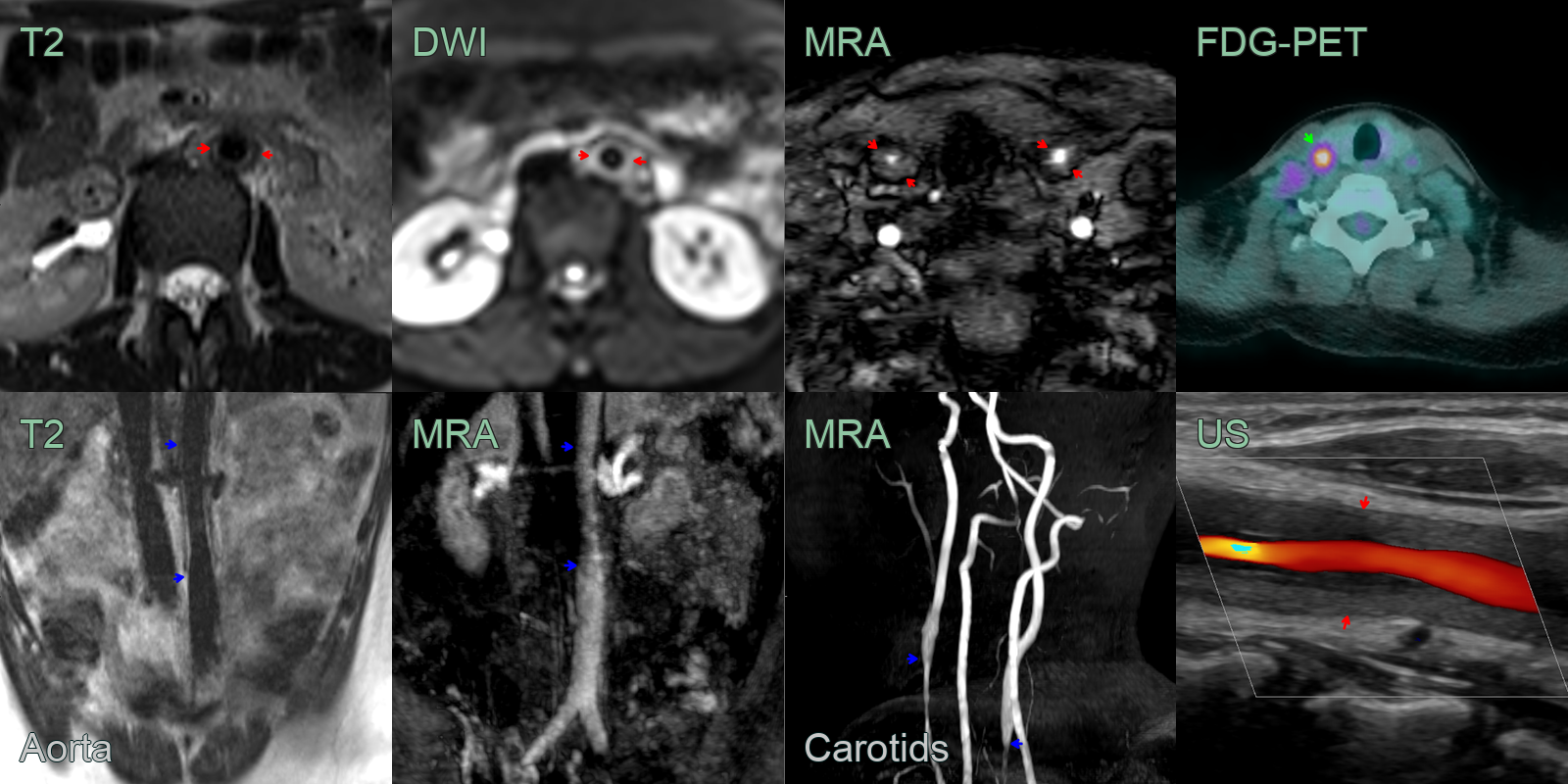
- 15-year-old patient presented with raised inflammatory markers and weight loss.
- The aortogram showed mural thickening (red arrows) and a 50% narrowing of the infrarenal aorta (blue arrows).
- Carotid angiography and Doppler ultrasound showed mural thickening (red arrows) and 70% stenosis (blue arrows) of the common carotid arteries.
- The areas of maximum carotid stenosis were avid on FDG PET.
- Intracranial arteries and brain perfusion was normal.
Treatment¶
- Corticosteroids and immunosuppression/biologics; revascularisation for critical stenosis. Circumferential wall thickening/enhancement of the aorta and its branches in a young woman is the key, with FDG-PET showing activity
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Giant Cell Arteritis | Predominantly involves temporal, vertebral, and ophthalmic arteries; cranial predilection rather than aortic arch; no subclavian involvement |
| Fibromuscular Dysplasia | "String of beads" alternating narrowing and dilatation on angiography; primarily affects renal and cervical arteries; no wall thickening on MRI |
| Atherosclerosis | Eccentric calcified plaques on CTA; diffuse large vessel involvement without circumferential wall thickening |
| Syphilitic Aortitis | Aortic root dilatation and aneurysm formation; coronary ostial involvement; similar vessel wall thickening to Takayasu |
| Kawasaki Disease | Coronary artery aneurysms on echocardiography/CTA; coronary predilection rather than aortic arch |
-
Somashekar et al. Updates in the diagnosis and management of Takayasu's arteritis. 2023. Postgraduate medicine - Open in new tab. ↩