Vein of Galen malformation¶
Summary
- Rare congenital cerebrovascular anomaly characterised by arteriovenous shunting into a dilated median prosencephalic vein of Markowski
- Presents in neonates or infants with high-output cardiac failure, macrocephaly, or seizures
- Diagnosis relies on neuroimaging, with treatment typically involving endovascular embolization1
Pathophysiology¶
- Abnormal connection between cerebral arteries and embryonic precursor of vein of Galen (median prosencephalic vein)
- Results in high-flow arteriovenous shunt
- Leads to:
- Venous hypertension
- Increased cardiac output
- Potential hydrocephalus due to venous outflow obstruction
Demographics¶
- Incidence: 1 in 25,000 live births
- Accounts for 30% of paediatric vascular malformations
- Male to female ratio: 2:1
- Usually diagnosed prenatally or in early infancy
Diagnosis¶
- Clinical presentation:
- Neonates: high-output cardiac failure, pulmonary hypertension
- Infants: macrocephaly, hydrocephalus, seizures
- Older children: developmental delay, headaches
- Physical examination:
- Cranial bruit
- Prominent scalp veins
- Signs of congestive heart failure
Imaging¶
- Ultrasound:
- Antenatal: dilated midline vascular structure posterior to third ventricle
- Postnatal: colour Doppler shows high-flow vascular malformation
- CT:
- Dilated vein of Galen
- Potential hydrocephalus or parenchymal calcifications
- MRI and MRA:
- Gold standard for detailed evaluation
- Demonstrates feeding arteries, nidus, and venous drainage
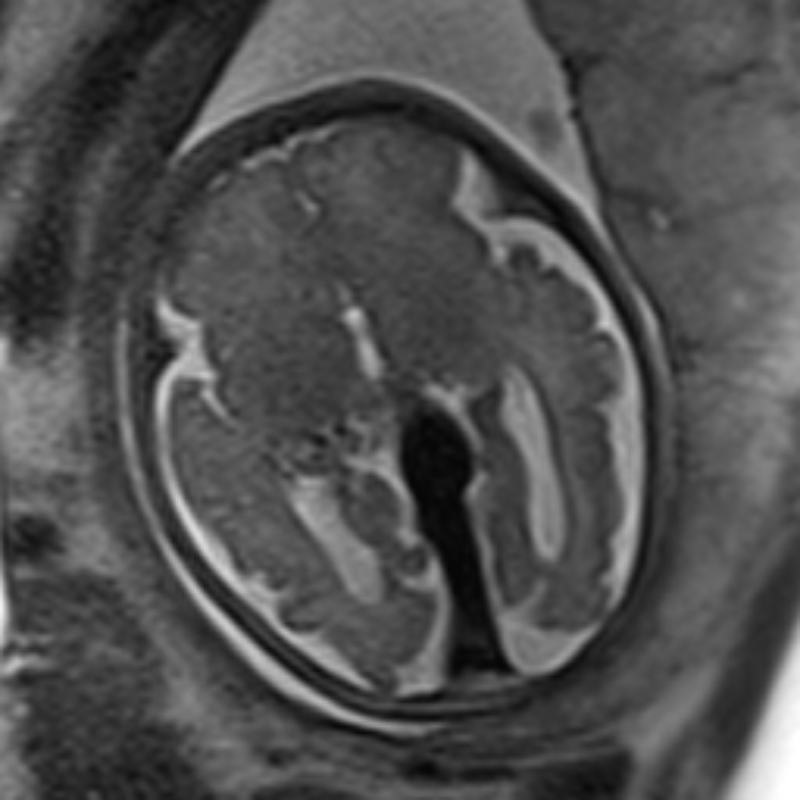
- T2-weighted images show flow voids
- Time-of-flight MRA delineates arterial feeders
- Cerebral angiography:
- Definitive imaging modality
- Essential for treatment planning
- Classifies malformation (choroidal or mural type)
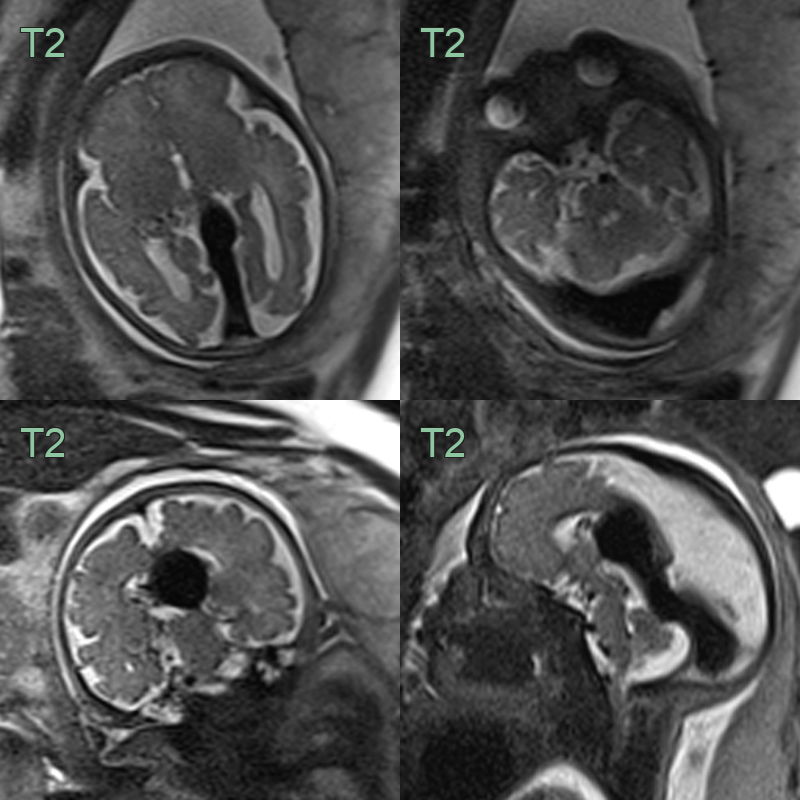
- Fetal MRI showed a gross dilatation of the vein of Galen and the transverse sinuses.
Treatment¶
- Staged endovascular embolisation, with management of high-output cardiac failure in neonates. The dilated midline median prosencephalic vein with arteriovenous shunting is the diagnostic finding
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Arachnoid cyst | Lacks flow voids on MRI; no arteriovenous shunting |
| Pineal region tumour | Solid mass rather than vascular structure; no arteriovenous shunting |
| Choroid plexus papilloma | Intraventricular location; solid, enhancing mass |
| Arteriovenous malformation | Nidus of abnormal vessels; usually not midline |
| Aneurysm of the vein of Galen | Single dilated vein without arteriovenous shunting |
| Dural sinus malformation | Involves dural sinuses; slower flow dynamics |
| Porencephalic cyst | Fluid-filled cavity in brain parenchyma; no vascular component |
| Hydrocephalus | Ventricular dilatation without vascular malformation |
| Subdural haematoma | Extra-axial collection; no vascular malformation |
| Sturge-Weber syndrome | Leptomeningeal angiomatosis; cortical calcifications |
-
Duran et al. Human genetics and molecular mechanisms of vein of Galen malformation. 2018. Journal of neurosurgery. Pediatrics - Open in new tab. ↩