Wilson's Disease¶
Summary
- Autosomal recessive disorder of copper metabolism
- Characterised by excessive copper accumulation in various organs, primarily liver and brain
- Imaging findings include basal ganglia abnormalities and hepatic cirrhosis1
Pathophysiology¶
- Caused by mutations in ATP7B gene on chromosome 13
- Impaired biliary copper excretion
- Reduced incorporation of copper into ceruloplasmin
- Results in toxic accumulation of copper in liver, brain, cornea, and other organs
Demographics¶
- Worldwide prevalence: 1 in 30,000 to 1 in 100,000
- No gender predilection
- Higher prevalence in certain populations (e.g., Sardinia, Eastern Asia)
Diagnosis¶
- Clinical presentation:
- Hepatic dysfunction
- Neurological symptoms (e.g., tremor, dysarthria, dystonia)
- Psychiatric disturbances
- Kayser-Fleischer rings in cornea
- Laboratory findings:
- Low serum ceruloplasmin
- Elevated 24-hour urinary copper excretion
- Elevated hepatic copper concentration on liver biopsy
- Genetic testing for ATP7B mutations
Imaging¶
- MRI:
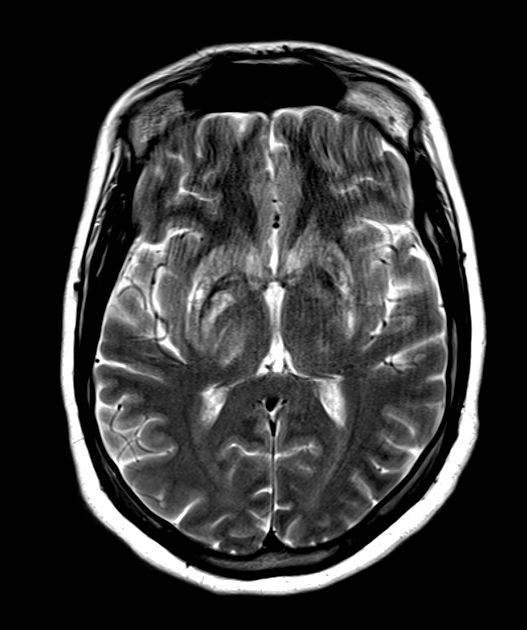
- Bilateral symmetric T2/FLAIR hyperintensity in the putamen, globus pallidus, caudate, thalamus and midbrain/pons
- "Face of the giant panda" sign in the midbrain (and a "panda cub" in the pons)
- T1 hyperintensity of the globus pallidus (from associated liver disease/manganese)
- SWI hypointensity from copper and iron deposition
- Generalised and brainstem atrophy in chronic disease
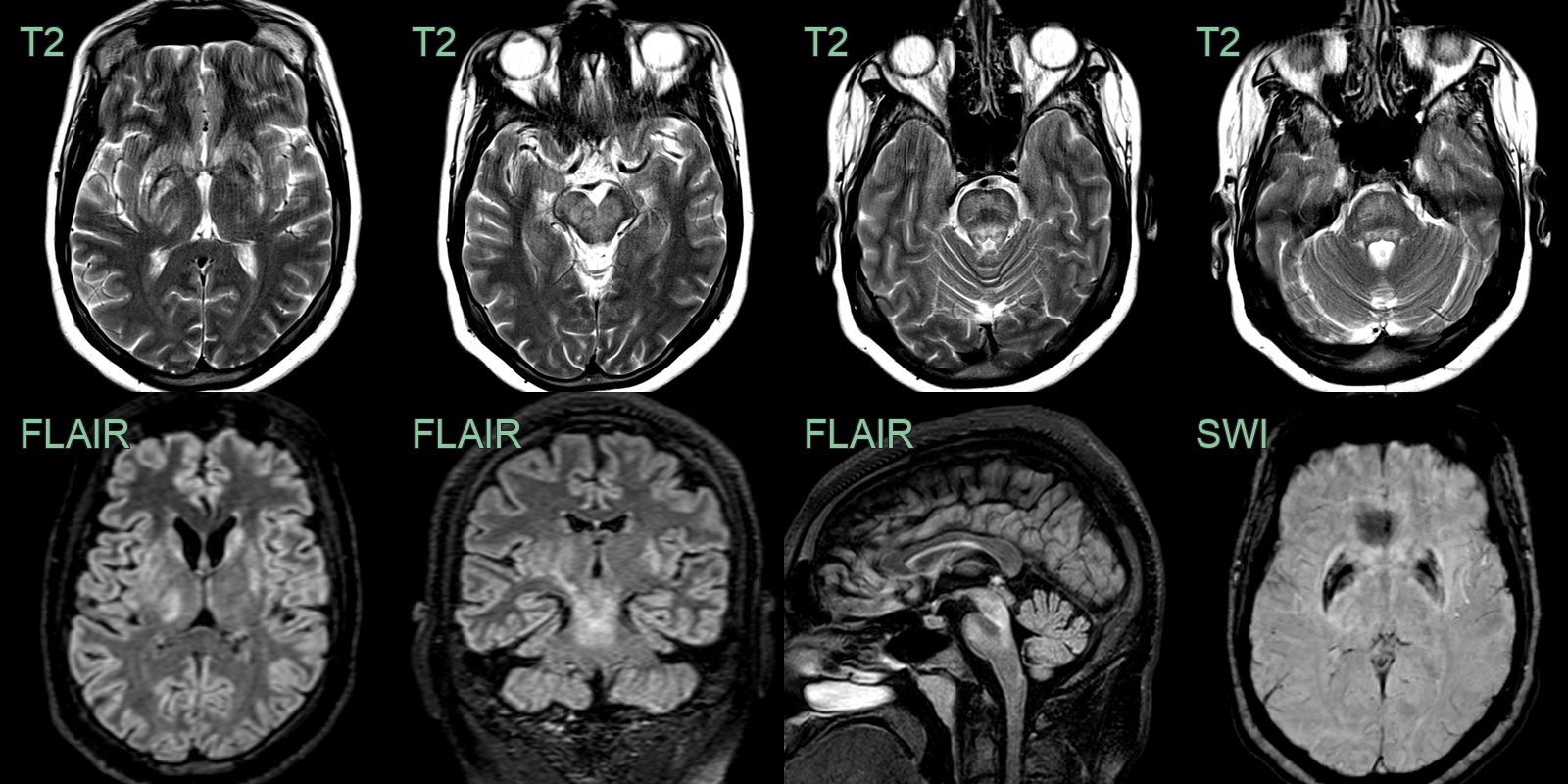
- A 25-year-old male presented 6 months prior with dysarthria, dystonia and cirrhosis.
- Imaging showed patchy hyperintensity in the deep grey nuclei and brainstem.
- SWI showed hypointensity in the globi pallidi.
Treatment¶
- Copper chelation (penicillamine/trientine) and zinc; liver transplantation for hepatic failure. The "face of the giant panda" midbrain sign is the classic imaging clue
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Acquired hepatocerebral degeneration | Bilateral symmetric T1 hyperintensity of globi pallidi; T2 hyperintensity in basal ganglia and white matter; no SWI hypointensity in copper-specific distribution |
| Leigh disease | Symmetric T2 hyperintensity in basal ganglia and brainstem periaqueductal grey; putamen and caudate involvement; no SWI hypointensity |
| Japanese encephalitis / flaviviral encephalitis | Bilateral thalamic and basal ganglia T2 hyperintensity; may show haemorrhage and restricted diffusion |
-
Bandmann et al. Wilson's disease and other neurological copper disorders. 2015. The Lancet. Neurology - Open in new tab. ↩