Cytotoxic Lesion of the Corpus Callosum¶
Summary
- Rare, reversible white matter lesion affecting the corpus callosum
- Characterised by transient oedema without infarction or necrosis
- Typically associated with various metabolic, infectious, or toxic etiologies1
Pathophysiology¶
- Exact mechanism unclear, but thought to involve:
- Cytokine-mediated inflammatory response
- Excitotoxicity due to glutamate release
- Oxidative stress and mitochondrial dysfunction
- Lesions predominantly affect oligodendrocytes and myelin
- Reversible oedema without true infarction or necrosis
Demographics¶
- Can affect all age groups, but more common in adults
- Slight male predominance reported in some studies
- Associated conditions include:
- Alcohol abuse and withdrawal
- Malnutrition
- Infections (e.g., influenza)
- Metabolic disturbances (e.g., hyponatremia)
- Drug toxicity (e.g., antiepileptics, chemotherapy)
Diagnosis¶
- Clinical presentation:
- Altered mental status
- Seizures
- Dysarthria
- Gait disturbances
- Laboratory findings:
- Often nonspecific
- May reflect underlying etiology (e.g., hyponatremia, elevated liver enzymes)
- Diagnosis primarily based on characteristic imaging findings
Imaging¶
- MRI is the modality of choice:
- T2-weighted and FLAIR: Hyperintense lesions in corpus callosum
- DWI/ADC: Restricted diffusion in acute phase
- T1-weighted: Hypointense to isointense lesions
- Contrast enhancement: Usually absent
- Typical distribution:
- Splenium most commonly affected
- Can involve entire corpus callosum in severe cases
- Key features:
- Symmetric, oval-shaped lesions
- No mass effect
- Reversible nature (resolution on follow-up imaging)
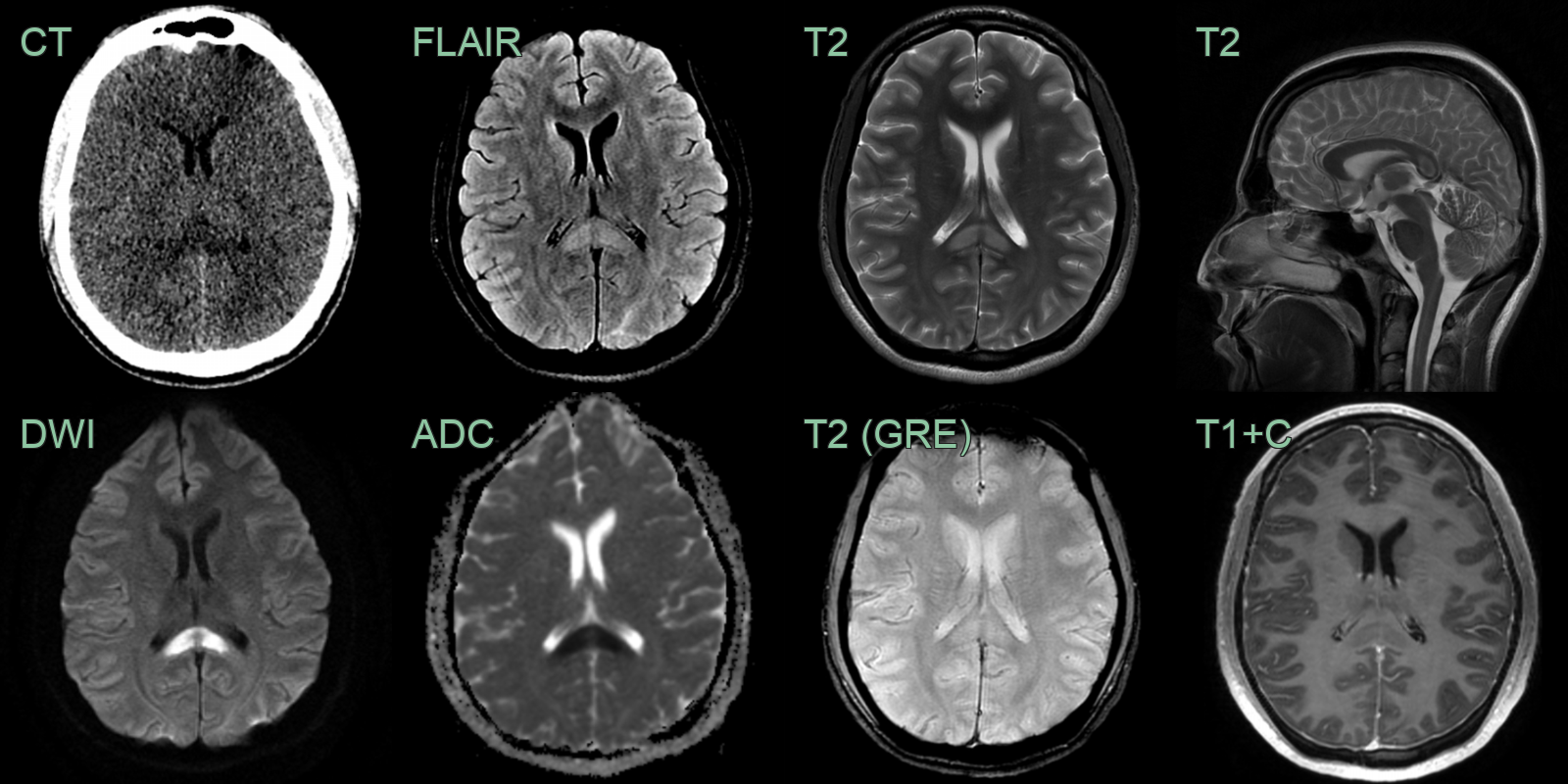
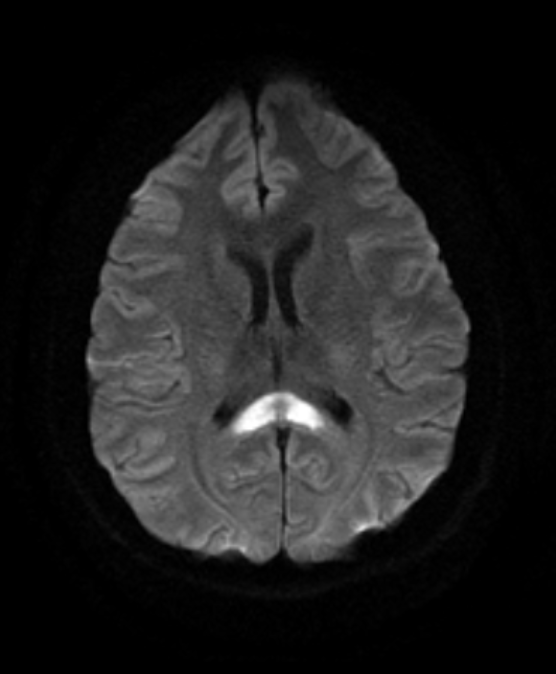
- 40-year-old patient with longterm epilepsy had his anti-epileptic medication changed following an increase in seizure frequency.
- CT showed low density in the splenium of the corpus callosum.
- On MRI, there was T2-hyperintensity and diffusion restriction in the same region.
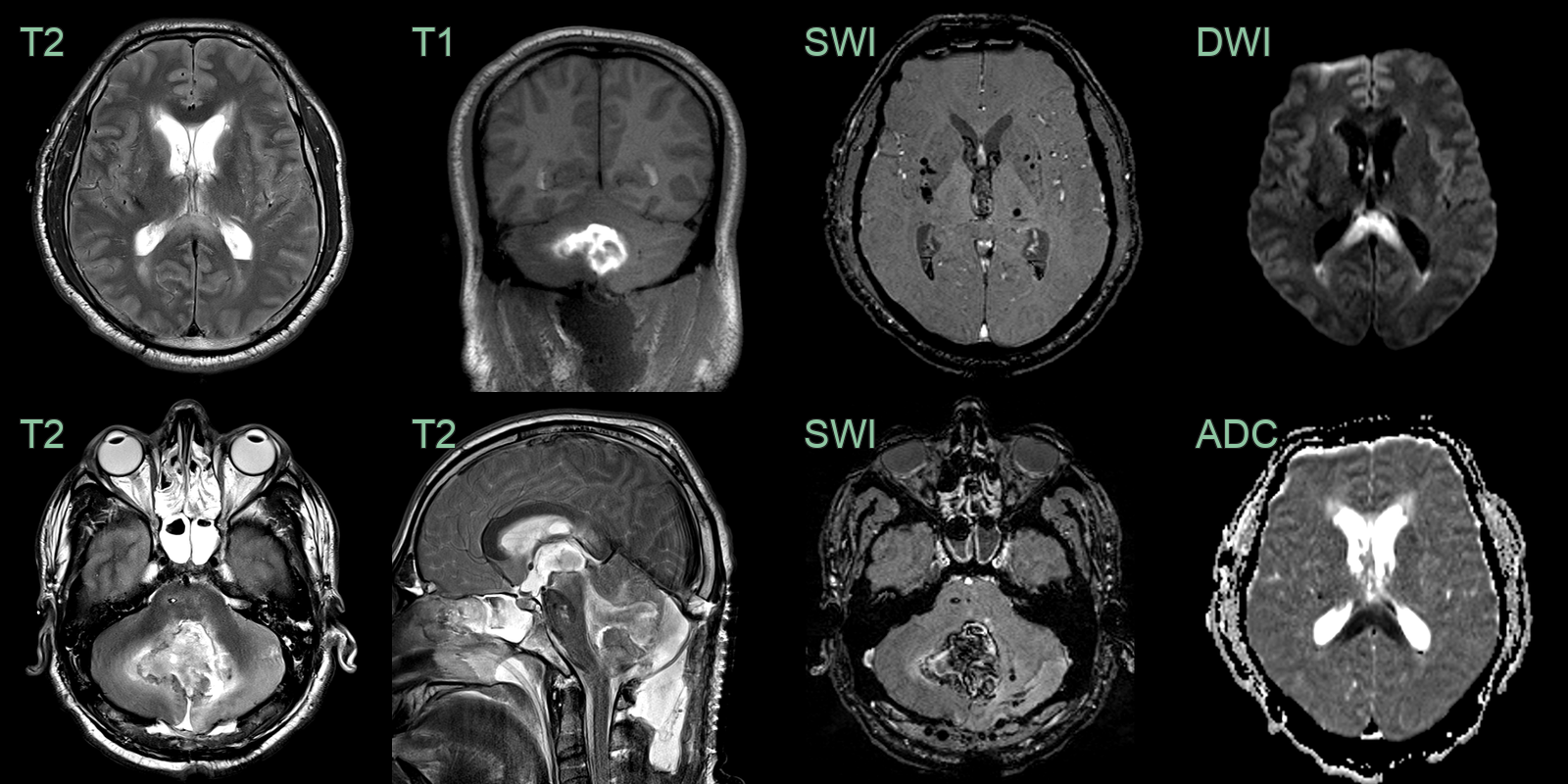
- A 50-year-old patient underwent a suboccipital decompression due to a posterior fossa haematoma.
- The presence of deep microhaemorrhages suggested that the haemorrhage was a consequence of hypertension.
- The symmetrical diffusion restriction within the splenium of the corpus callosum was compatible with a CLOCC.
Treatment¶
- Treat the underlying cause; the lesion is typically reversible and resolves on follow-up
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Multiple Sclerosis | Lesions typically ovoid and periventricular; less likely to involve entire corpus callosum |
| Acute Disseminated Encephalomyelitis | More widespread brain involvement; usually monophasic |
| Ischaemic Stroke | Arterial ischaemia usually unilateral (venous ischaemia could be bilateral); diffusion restriction more pronounced and persistent |
| Posterior Reversible Encephalopathy Syndrome | Predominantly affects posterior cerebral regions; often spares corpus callosum |
| Marchiafava-Bignami Disease | Primarily affects alcoholics; involves entire corpus callosum more uniformly |
| Wernicke Encephalopathy | Involves mammillary bodies, thalami, and periaqueductal gray matter |
| Viral Encephalitis | Often involves temporal lobes; may have meningeal enhancement |
| Vasculitis | Multiple infarcts of different ages; vessel wall enhancement may be seen |
-
Lebecque et al. Cytotoxic Lesion of the Corpus Callosum Caused by Puumala Hantavirus Infection. 2019. Journal of the Belgian Society of Radiology - Open in new tab. ↩